
Submitted by jer5150 on Sun, 07/01/2012 - 10:58

- Sometimes less is more! I've overhauled this blog by streamlining it's content and creating a shorter version. We'd love to hear your feedback.
This week's entry is courtesy of guest contributor, fellow blogger, and ECG Guru member DrArnel. My first direct contact with Dr. Arnel Carmona was back on May 28th of this year. At the encouragement of Dr. Ken Grauer, I decided to email Arnel with the intent of expressing my alternate interpretations of the rhythms seen above. In his reply to me, Arnel was very receptive and has even gone on to share these tracings with Dr. Kyunhyun Wang. I've taken the liberty of editing and paraphrasing Arnel's original comments in an attempt to summarize this case study without divulging the answer. In the interest of obtaining a "gold-standard" diagnosis, it should be noted that Arnel had these tracings professionally vetted by a cardiologist who specializes in cardiac electrophysiology (EP). These represent arrhythmias seen in the context of a background of drug use.
Patient’s clinical data: 50-year-old man who came in with dizziness/ (? syncope) with high BP, diaphoretic and irregular heart rate. Heart rate started in the upper 50's to upper 60's. Then at the strike of 1200 midnight these rhythms appeared.
The bedside nurse was so concerned because the patient was so diaphoretic.
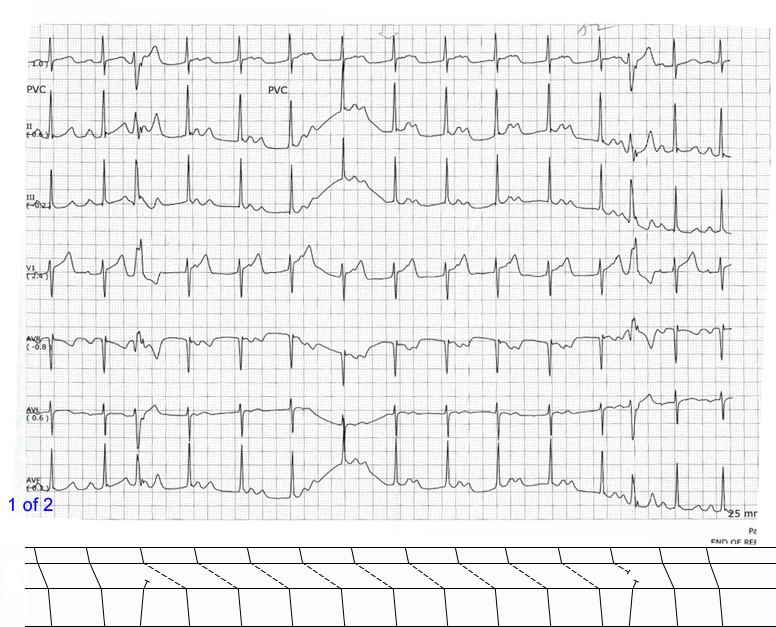
Later this rhythm appeared in tracing 1 of 2.
The on-call MD was called. At this point the bedside nurse called for a rapid response consult.
Then later: 2 of 2.
So the critical care MD came and patient was started on isoproterenol drip. The other labs came and drug screen came with positive for amphetamines and cannabis. Amphetamine can explain the hypertension and diaphoresis.
Update-
The isoproterenol did well. The next day the drip was tapered but the rhythm changed recurred. Also it was found out that the patient had a big cerebellar infarct producing the syndrome pseudotumoral cerebellar infarction.
On day 1 the patient was transferred to ICU and intubated due to the neuro condition. The rhythm problems did not recur.
- Question: What mechanism of conduction is this illustrating?
Hint # 1: I've constructed "simplified" laddergrams directly underneath both of the rhythm tracings. In the A-V tier, note the two different styles of oblique lines. There are solid lines (i.e., ––––––––– ) and there are broken/dashed lines (i.e., - - - - - - - - ).
Hint # 2: In tracing 1 of 2, the 3rd and 13th beats are unifocal ventricular premature beats (VPBs). The first VPB is interpolated and interrupts an otherwise regular rhythm and triggers a prolongation of the P-R interval. A few seconds later the second VPB reverts the P-R interval back to its normal baseline appearance. In tracing 2 of 2, the spontaneous prolongation of the P-R interval is not triggered by a VPB. Both of these tracings look nearly identical to ones I've seen both personally in my clinical career as well as tracings I've seen in publications by Dr. Charles Fisch.
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
INTERPRETATION
The conduction mechanism responsible for causing the alternating lengths of the P-R intervals is what's known as Dual A-V Nodal Conduction. Atrioventricular (A-V) conduction is alternating between the A-V node's fast pathway (FP) and the slow pathway (SP). In the bottom ECG it appears to happen spontaneously however in the top ECG the onset and offset are triggered by isolated VPBs (3rd and 13th beats). Both of these ECGs bear a striking similarity to the ones published in Chapter 17 of Dr. Charles Fisch's textbook "Electrocardiography of Clinical Arrhythmias." Honestly, I never heard of Dual A-V Nodal Conduction until I read Dr. Fisch's textbook. This book was one of the few that Dr. Henry J. L. Marriott recommended in the front of his book Rhythm Quizlets.
In the laddergram's A-V tiers, the solid lines (i.e., ––––––––– ) represent conduction via the FP and the broken / dashed lines (i.e., - - - - - - - - ) represent conduction via the SP.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]