
Submitted by Dr A Röschl on Sat, 05/27/2023 - 01:46
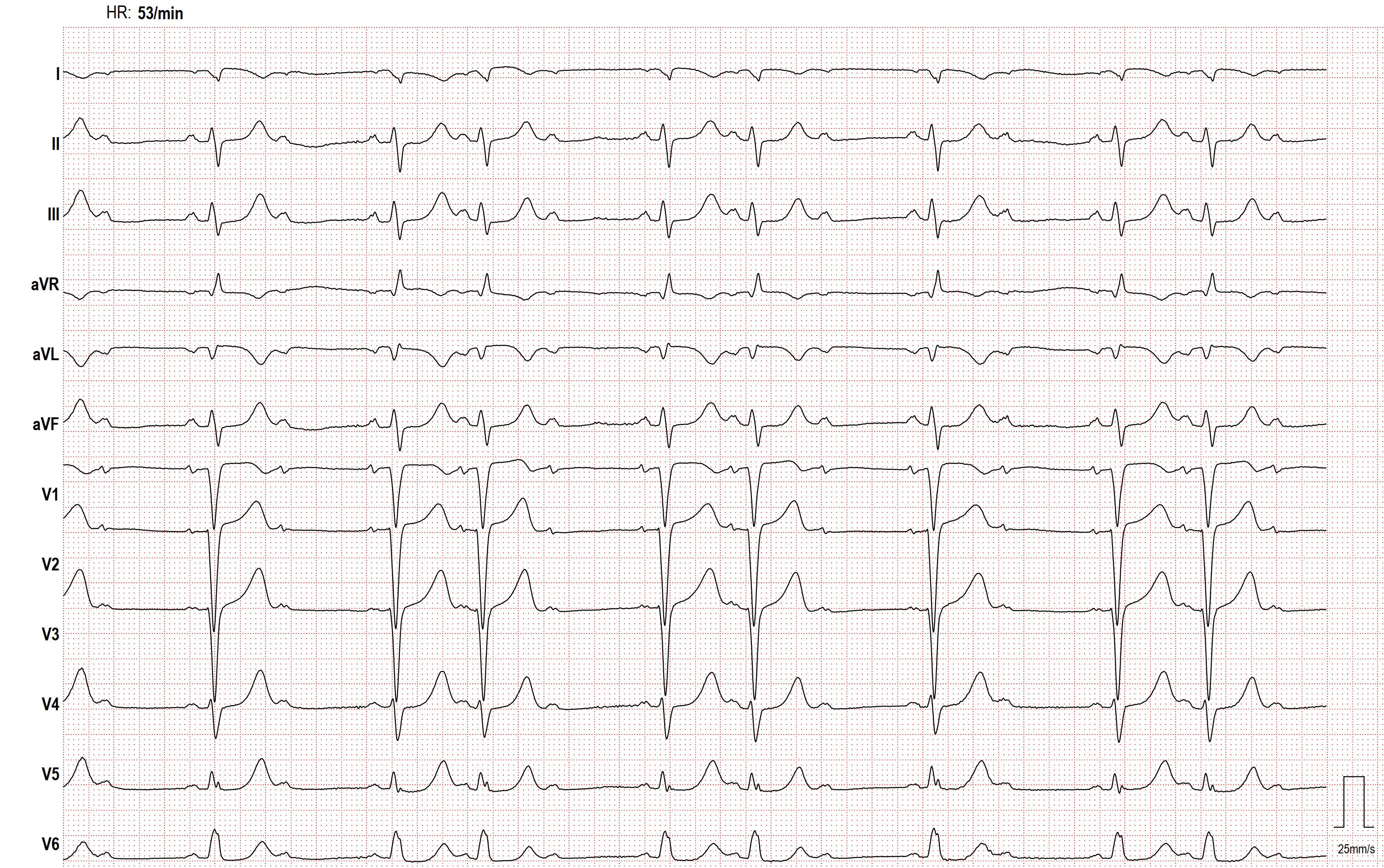
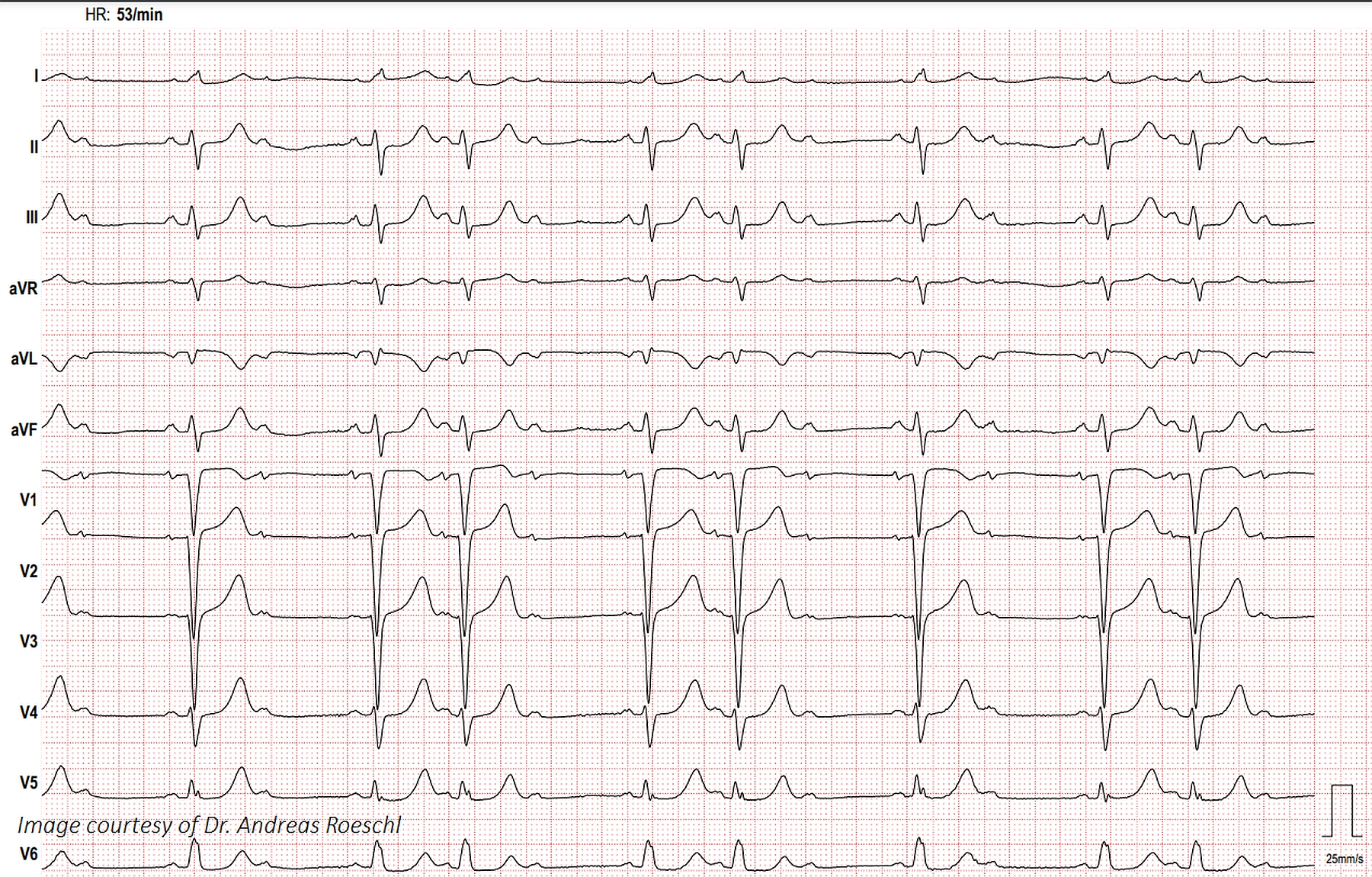
This ECG shows second-degree AV block, Mobitz Type II and an interventricular conduction delay, probably left bundle branch block. The QRS width is about 130 ms, or .13 seconds. The first ECG was run with the right and left arm electrodes reversed, so we cannot demonstrate the usual criteria of LBBB: Wide QRS, Supraventricular rhythm, V1 negative deflection and Leads I and V6 with positive deflections. When the arm electrodes are reversed, Lead I becomes negative, Leads II and III switch places, and Leads aVL and aVR switch places. The second ECG demonstrates the arm electrodes in the correct position, and LBBB criteria met.
In second-degree AVB, Type II, there is almost always ECG evidence of fascicular disease such as right bundle branch block or left bundle branch block, as Type II is most often an intermittent tri-fascicular block. That is, one or two fascicles of the bundle branches are completely blocked, and the remaining one or two fascicles are intermittently blocked. So, in this case, the left bundle branch (two fascicles) is blocked, and the right bundle branch (one fascicle) is intermittently blocked. At the moment all three fascicles are blocked, there is complete heart block. So, we could say that second-degree AVB, Type II is an intermittent trifascicular block, or intermittent complete AV block.
Rate this content:
-

- Dr A Röschl's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.