
Submitted by Dawn on Fri, 10/19/2012 - 20:46
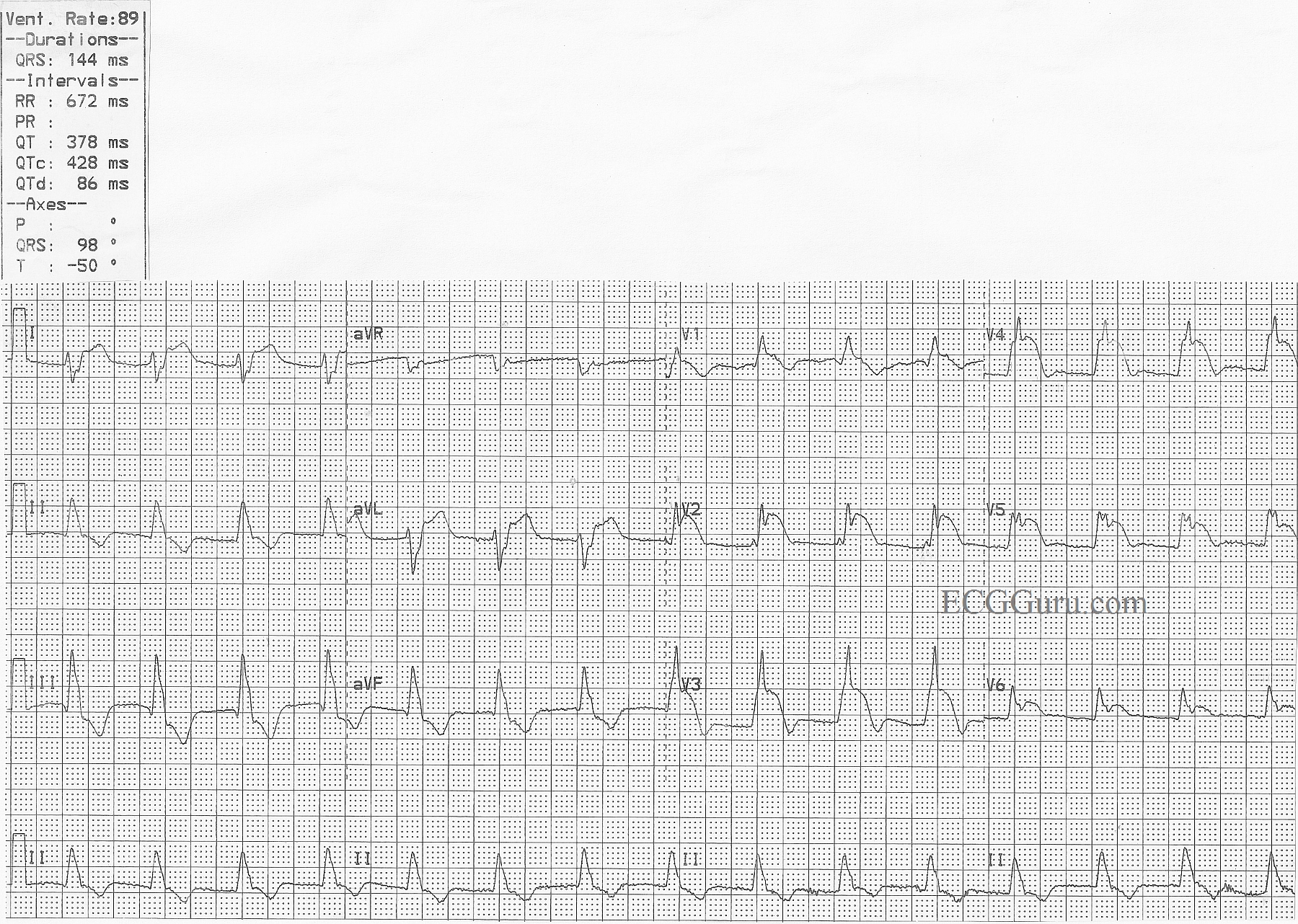
This is a good example of acute anterior wall M.I., with ST elevation in V1 through V6, as well as in Leads I and aVL. The extensive distribution of ST segment elevations across the anterior and high lateral walls indicates a proximal LAD artery occlusion. In addition, this ECG shows right bundle branch block, with a QRS width of 144 ms (.14 sec.) and an rsR' pattern in V1. There is also a wide s wave in Lead I which is partly obscurred in V6 by the ST elevation. The right axis deviation (98 degrees) suggests a left posterior fascicular block which, when coupled with the RBBB, is a bi-fascicular block. P waves are difficult to see. Do you think they are found at the end of the QRS complexes, representing a long first-degree AVB? Look at leads V3 through V6 for clues.
Please feel free to add your comments below. The more "gurus" the better.
A good ECG to teach your students that a patient facing a life-threatening emergency may have a "normal" rate and regular rhythm. There is something in this ECG for beginners through advanced students.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Can't miss that one!
Great ECG there!
Even the novice could not miss that MI, but would they pick up the bifascicular block?
Jamie Bisson
http://www.eadvancedhealthcare.com/healthcare-resources/ecg-interpretati...
Big MI!- but What is the Rhythm?
Nice illustrative example by Dawn - with a number of teaching points:
For anyone interested - I've made a site to assist in localization of the MI and identification of the culprit vessel. GO TO: https://www.kg-ekgpress.com/ecg_-_coronary_anatomy-mi_localization/
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Rhythm question
Thanks, Dr Ken, for your great teaching points. We wish we had a long rhythm strip. It's frustrating to be unsure of the rhythm, but the danger is clear for this patient, as you pointed out. I encourage all instructors and students to follow Dr Ken Grauer's link to his information on localizing MIs
Dawn Altman, Admin