
Submitted by Dawn on Tue, 07/12/2016 - 16:00
This ECG is from a 46-year-old woman with diabetes mellitus. She presented to the Emergency Dept. with a complaint of weakness. Her BP was elevated at 186/102. Her blood glucose was 936 mg/dL (normal 70-105).
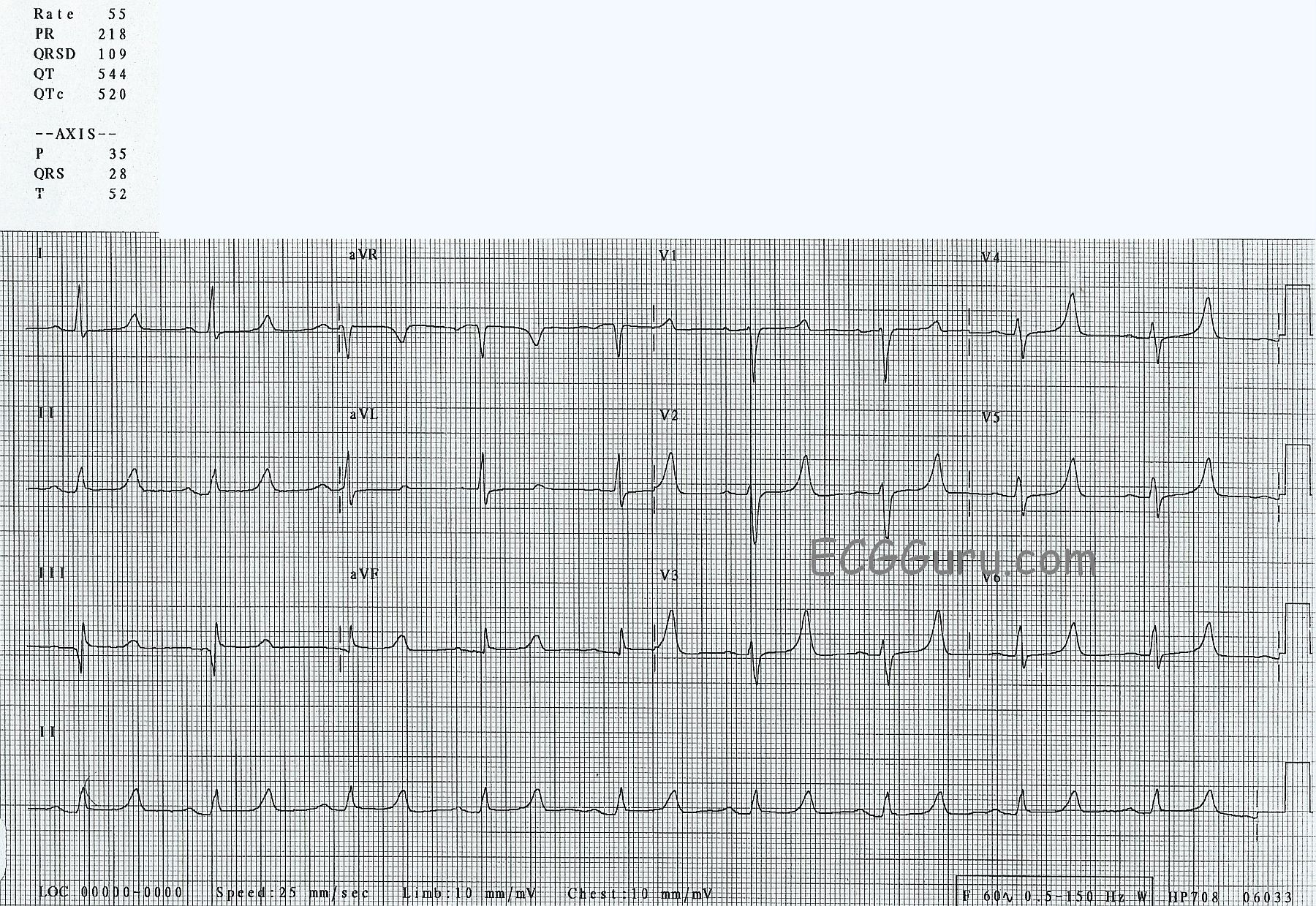
So, what does her ECG show?
1) Sinus bradycardia at 55 bpm. The rhythm is regular, with no extrasystoles.
2) A slightly prolonged PR interval at 218 ms (.218 seconds). Normal is 120-200 ms.
3) A “wide side of normal” QRS duration at 109 ms. Normal is 70-100, but can be a little longer in normal individuals.
4) A prolonged QTc interval at 520 ms. Normal QTc is 460 ms or less in women. A helpful rule of thumb is that the QT should be less than half the preceding RR.
5) Normal P waves.
6) Normal axes of P, QRS, and T waves.
7) A large Q wave in Lead III which is not repeated in aVL. This can be inconsequential when confined to Lead III, or can be a pathological Q wave, especially if also seen in aVF.
8) Flat ST segments. Normal ST segments are convex upward, like a smile.
9) Tall, peaked T waves in precordial leads V2 through V6, and in Lead II.
What does it mean?
Unfortunately, we do not have complete labs for this patient, or any information about her outcome.
We know that patients who have uncontrolled diabetes are at risk for renal failure, so we should consider electrolyte imbalances when we see abnormalities in the ECG.
The prolonged, flat ST segment is suggestive of HYPOCALCEMIA. The low-amplitude P waves and tall, peaked T waves suggest HYPERKALEMIA. You will find a discussion of simultaneous hypocalcemia and hyperkalemia on this website HERE.
We are looking forward to your comments.
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
An “Aunt Minnie” Tracing with a “High” and a “Low” …
There is an expression in radiology that a particular X-ray picture is an “Aunt Minnie”. By that it is meant that try as one may, it can be very difficult to describe in words what a particular person looks like (especially a dear but aging “Aunt Minnie” ) — however, once you get to see Aunt Minnie in person — you’ll never forget what she looks like!
So it is with this week’s Instructor ECG. All it should take is a brief glance at this tracing and, no more than a little history to “set the scene” for potential significant renal disease — and one should immediately recognize high probability of acute renal failure with combined hyperkalemia and hypocalcemia!
Initial ECG findings of Hyperkalemia are well known to any provider who regularly interprets ECGs: T waves in many leads become disproportionately tall and peaked. The image of such T waves resembles that of the Eiffel Tower — tall, peaked and pointed with a narrow base. As hyperkalemia becomes more severe — P wave amplitude decreases (and eventually the P wave may disappear), as the QRS complex progressively widens — until either ventricular fibrillation or asystole ensues. T waves in this tracing are characteristic of this initial stage of being tall, peaked and pointed with a narrow base (usually corresponding to a serum K+ value of ~ 6.0-7.5 mEq/L) — while P wave amplitude remains appropriate, and the QRS complex is no more than minimally widened.
ECG recognition of Hypocalcemia is more challenging — and in many cases, not recognizable from the ECG alone. The characteristic finding is QT prolongation with a long, flat ST segment that culminates in an otherwise unaffected T wave. The KEY — is to recognize that hyperkalemia and hypocalcemia commonly coexist with new renal failure. When they do, you will occasionally see the pathognomonic picture shown here — in which T waves are diagnostic of hyperkalemia, with these T waves occurring in association with obvious QT prolongation at the end of an isoelectric (flat) ST segment.
----------------------------------------------
For those who want to read more:
— CLICK HERE to download a pdf of my Section 11.0 (from my ECG-2014-ePub) — which reviews ECG recognition of Electrolyte Disorders.
Ken Grauer, MD www.kg-ekgpress.com [email protected]