
Submitted by Dawn on Sun, 03/17/2013 - 19:42
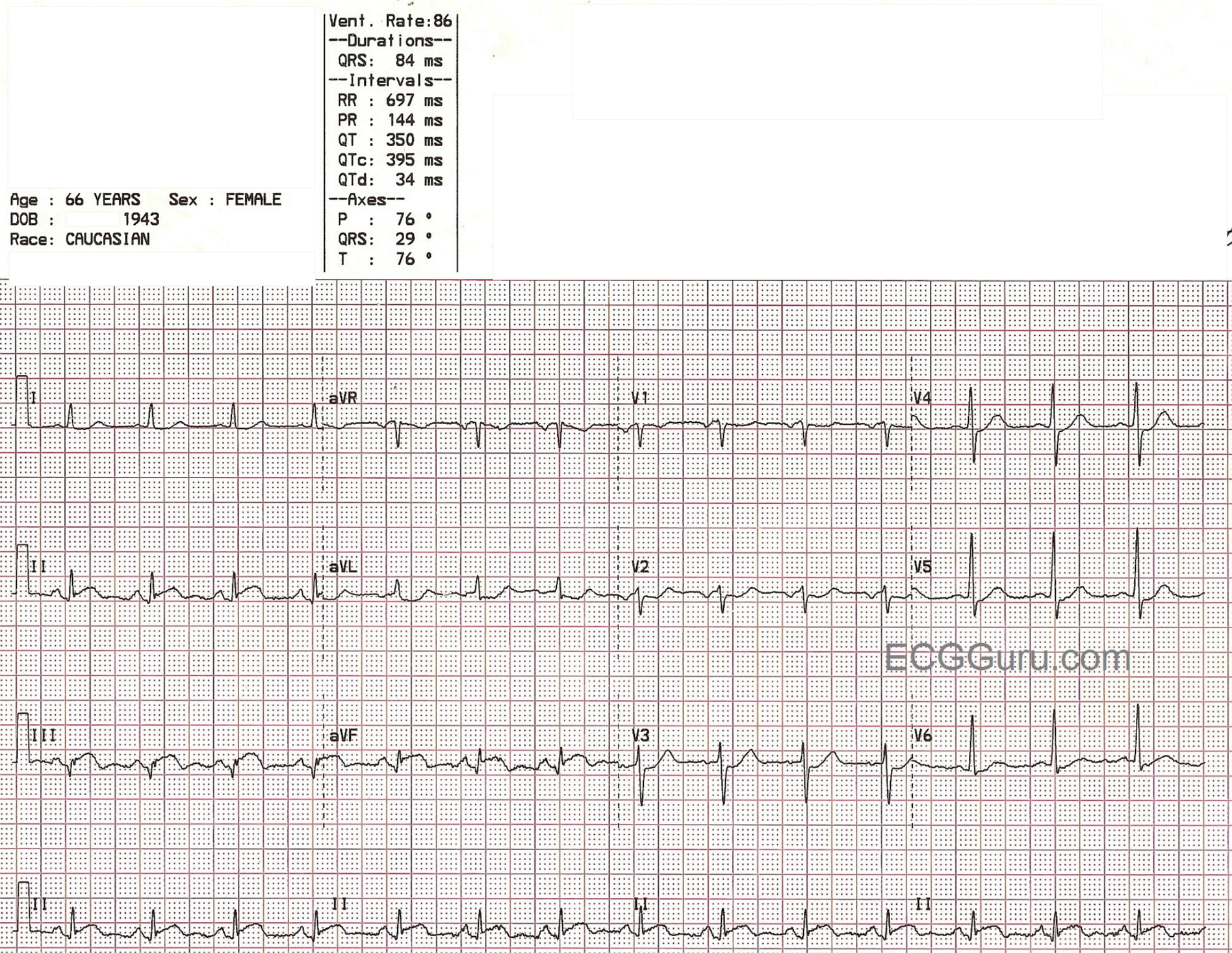

This ECG was taken from a 66-year-old woman who presented to the emergency department complaining of chest pain and shortness of breath. She attributed her symptoms to her COPD, but stated that her aerosol treatment had not helped. She waited for some time before deciding to go to the hospital, then drove herself. In the emergency department, she had blood drawn, an I.V. started, and an aerosol treatment of albuterol. She was then taken to the radiology dept. for a chest xray. When she returned, a 12-lead ECG was done. 45 minutes had passed since she first arrived at the hospital. This ECG is shown here. It shows ST elevation in the inferior leads: II, III, and aVF. The patient was taken immediately to the cath lab, where her right coronary artery was found to have a 100% occlusion. (See image accompanying this ECG). Angioplasty was successful, and stents were placed in the artery. The patient was found to have anemia, with a hemoglobin of 5.5, and she was given a blood transfusion. During the cath procedure, a ventriculogram was performed, which showed a stunned and akinetic inferior wall. Unfortunately, subsequent ventriculogram performed several weeks later showed the lack of motion of the inferior wall to be permanent. The ventriculogram is also posted here, and at this YouTube link, so you will be able to show your students the mechanical effects on the heart of a delay to treatment in acute STEMI. See our YouTube site for more ventriculograms and cath videos.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Acute Infero-Postero MI - Time Delay - SUPERB Teaching Case!
There are a number of important messages integrated in Dawn's Instructor ECG for this Week:
Ken Grauer, MD www.kg-ekgpress.com [email protected]