
Submitted by Dawn on Sun, 07/08/2012 - 20:34
When students are learning to recognize ST elevation M.I. (STEMI), they often want to know, "How many blocks does the ST segment have to be elevated for it to be a STEMI?". Counting blocks simply does not work. Depending on the experience level of your students, it is important to introduce other characteristics of the ST elevation.
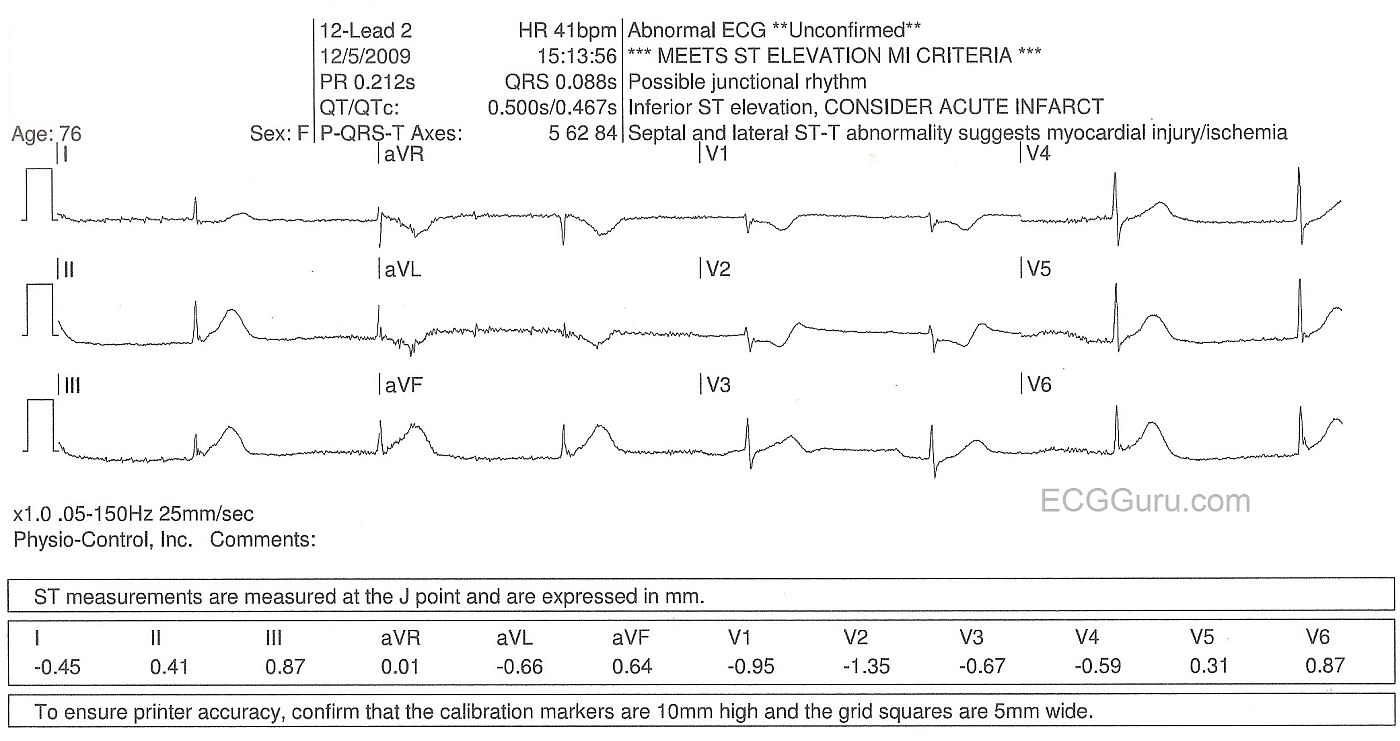
Even subtle elevations can indicate acute M.I. when other features are present. These include, ST elevation in related leads, a flat or coved upward ST segment, associated signs such as T wave inversion and pathological Q waves, reciprocal depressions, and of course patient presentation.
This ECG shows subtle ST elevations. The LifePak 15 (PhysioControl) has read it as "Meets ST Elevation MI Criteria". LifePak 15 uses the University of Glasgow criteria, which takes into consideration the age and gender of the patient, among other things. The paramedics who cared for this patient were confused because she had chest pain, and the LifePak said she had MI criteria, but they counted blocks and did not find 1 mm ST segment elevation as they were taught. To the experienced eye, of course, this ECG looks like the CLASSIC inferior wall MI, with the classic bradycardia (junctional rhythm) often seen. This patient was evaluated in the cath lab, and treated for acute STEMI.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
The big clue on this ECG is
The big clue on this ECG is the downsloping ST-depression in aVL! I think part of the failing in EMS 12-Lead education is the misnomer that ischemia localizes as ST-depression rather than searching for the reciprocal ST-elevation.
Great case!
Christopher
sixlettervariable.blogspot.com
ems12lead.com
Agreed
In nearly every class I teach, even when the audience consists of students I have taught before, a majority of paramedics will identify ST depression as "ischemia" in all cases! I am always taken aback, since I teach reciprocal changes every time I teach a STEMI class or a basic 12-lead class. People, by nature, like simple answers. They don't always want to hear, "This could be due to this, OR this, OR maybe even this".
Dawn Altman, Admin
HyperAcute T Waves - in this Infero-Postero-Lat MI
Excellent point made by Dawn that there is NO fixed "amount" of ST elevation needed to qualify as "enough for an acute MI". SHAPE counts more than amount. I'd add a number of additional points to this post:
Great example of acute MI despite a minimal "amount" of ST elevation!
Ken Grauer, MD www.kg-ekgpress.com [email protected]