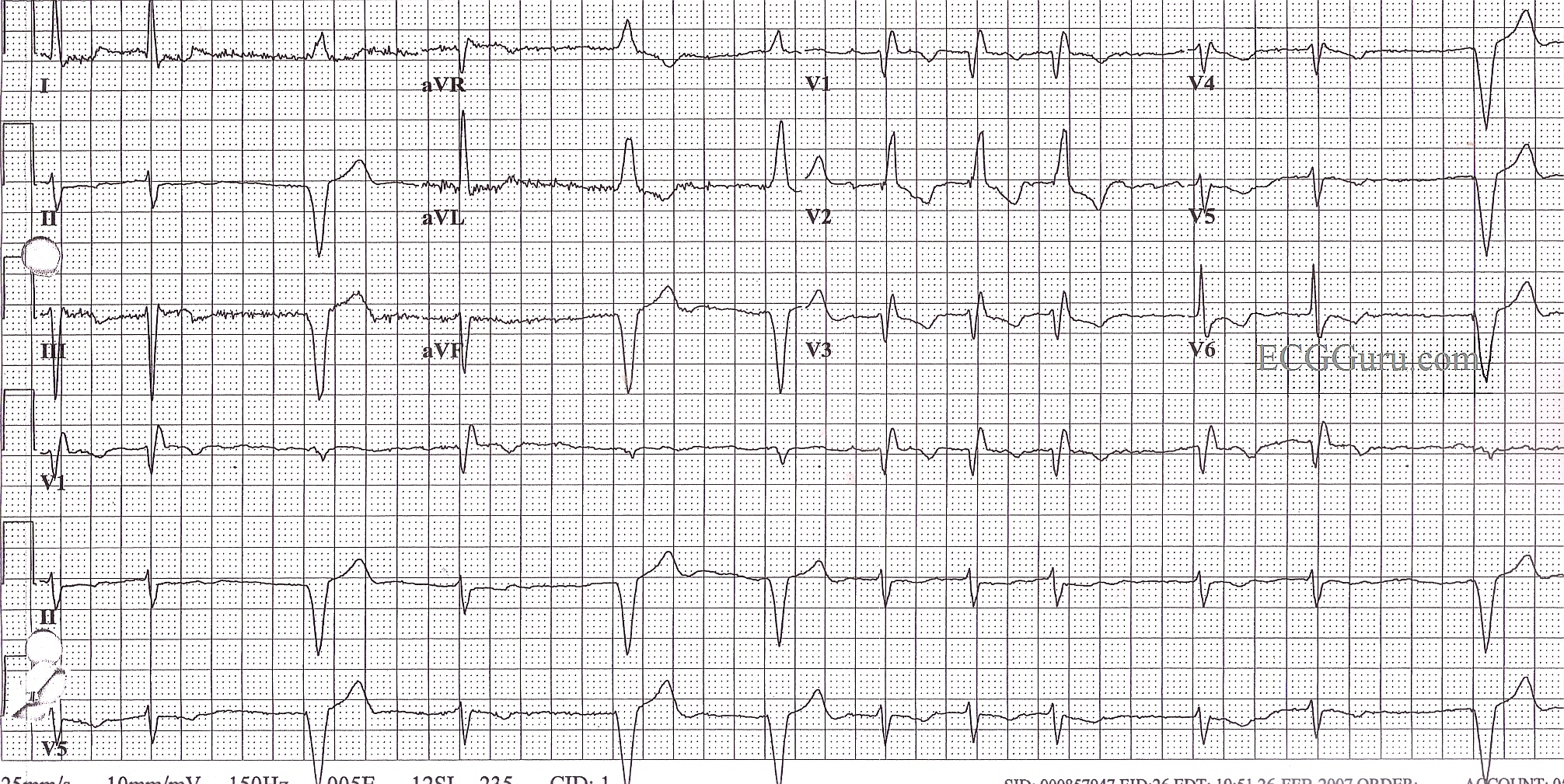
Lots of information in this ECG! The underlying rhythm is atrial fibrillation with a controlled rate. The QRS is .12 seconds in duration, with an rSR' pattern in V1 and a wide s wave in Leads I and V6, indicating right bundle branch block. In addition, the axis is leftward - Leads I and aVL are upright and Leads II, III, and aVF are negative. There is no other obvious reason for the left axis shift, and therefore, the diagnosis by exclusion is left anterior fascicular block. RBBB and LAFB often appear together, as the right bundle branch and the anterior fascicle of the left bundle share the same blood supply from the left coronary artery. ALSO, this patient has a right ventricular pacemaker, and is pacing appropriately when the atrial fib slows. Pacer spikes are not readily seen, but the width of the QRS, the axis of the wide QRS complexes (left), and the timing (after a pause) all support the paced rhythm diagnosis. V5 and V6 actually show a very tiny hint of a spike. The T wave inversions seen in the upright leads are common with RBBB, and are usually considered normal in this setting.