
Submitted by Dawn on Mon, 11/25/2013 - 01:26
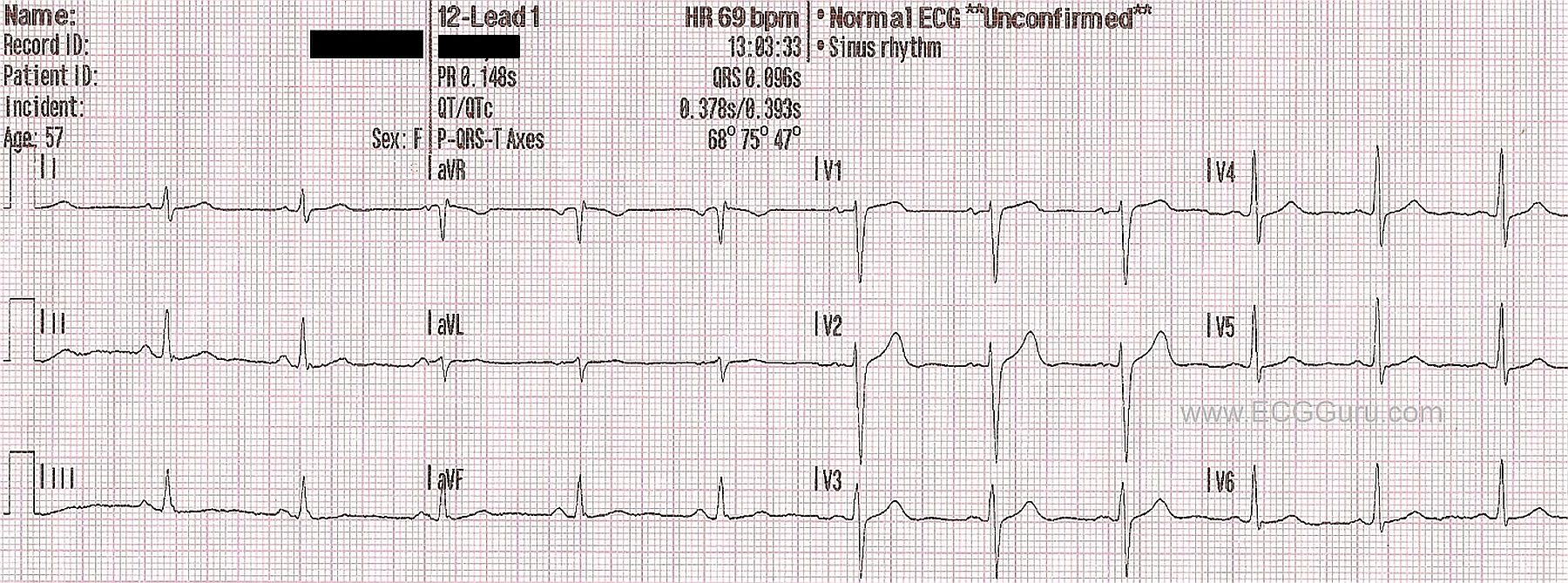
It is always good to have a number of "normal" ECGs in your collection. This particular ECG has only three channels, lacking the fourth channel that is usually used for a rhythm strip. Some of your students might not work in settings where they have access to four-channel ECG machines. Often, paramedics in the field and medical personnel who use "crash carts" have ECG machines with narrow paper that run three channels at once. They will print their rhythm strips on one sheet and the 12-lead on another. This poses a slight handicap when evaluating complex rhythms, but is adequate for most emergency ECG screenings.
This ECG has a number of features that your students should recognize as normal. The rate and intervals are within normal ranges. The ST segments are neither elevated or depressed. The axis of the frontal plane leads is normal, as is the R wave progression in the chest leads. The T waves are upright, and the P waves are uniform and upright in the inferior leads. The rhythm is sinus. There is no appreciable artifact.
A good understanding of what is "normal" is vital for recognizing "abnormal".
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Recognizing Normal
As per Dawn - it is highly instructive to periodically mix in "normal" ECGs with abnormal ones - since one of the major tasks of the health care provider is to be comfortable distinguishing the two. This is sometimes far easier said than accomplished - especially when the patient in question is acutely symptomatic. I'd add the following points to Dawn's presentation:
It is often instructive for learners to see how many comments they can make about normal ECGs.
Ken Grauer, MD www.kg-ekgpress.com [email protected]