
Submitted by Dawn on Thu, 04/18/2013 - 22:17
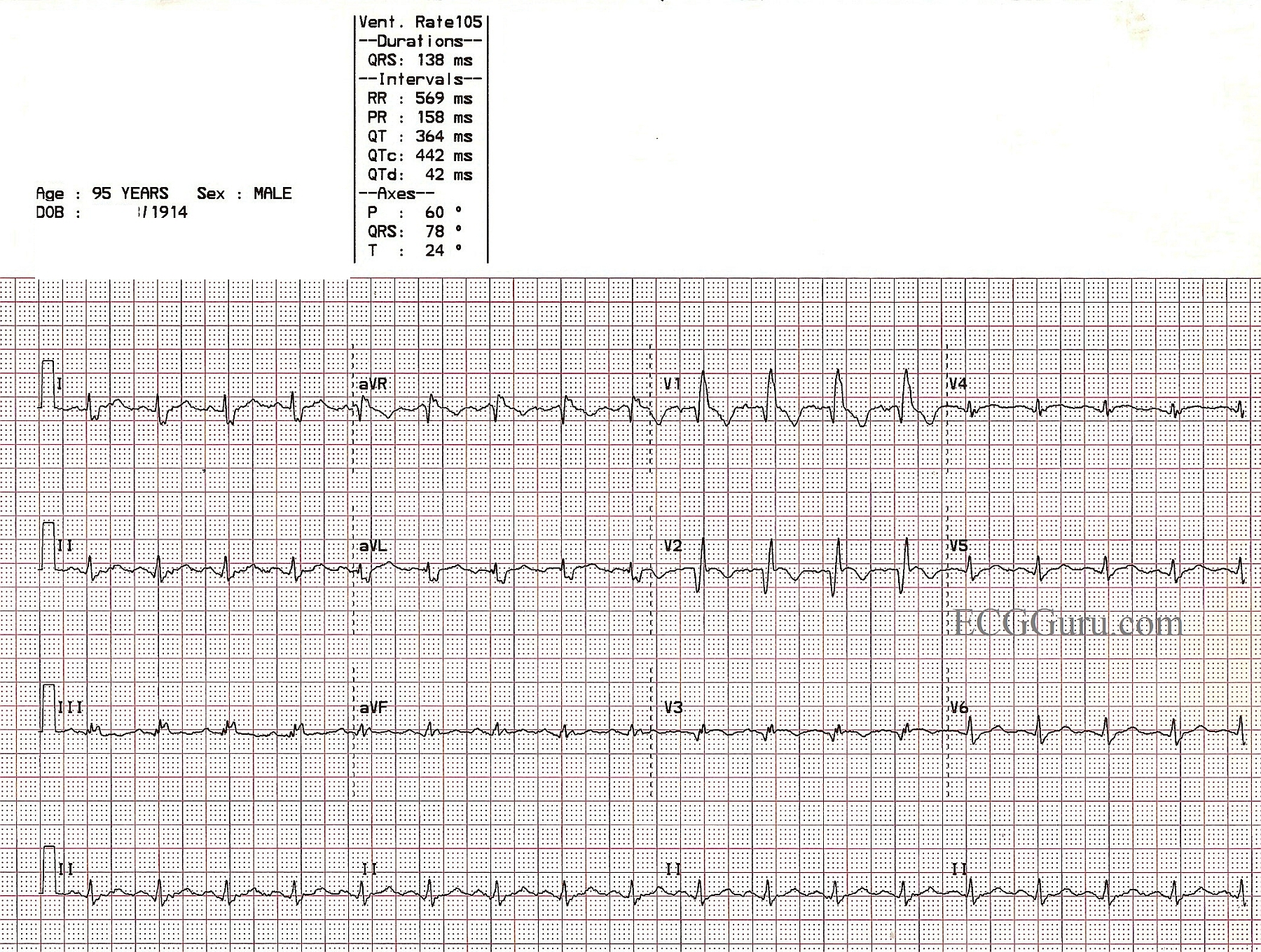
This is an ECG from a 95 year old man who was recovering from an anterior-septal wall M.I. Other clinical data for this patient has been lost, except that he suffered a new right bundle branch block during this M.I. The ECG shows pathological Q waves in V1, V2, and V3, consistent with permanent damage (necrosis) in the anterior septal wall. The ST segments in those leads are coved upward. Even though the J points are not elevated, this ST segment shape suggests recent injury. The classic RBBB pattern is present: wide QRS, rSR' pattern in V1, and wide little s waves in I and V6. It is not known why the overall voltage is low in this patient.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
RBBB and Recent Anterior MI - Recognizing the Infarct
Great example by Dawn of RBBB with ECG signs of recent acute MI. I'll add several points to Dawn's description:
Although it is more difficult to assess acute ischemia/infarction in the setting of QRS widening from BBB (Bundle Branch Block) - it will nevertheless be possible to do so in many cases. It is definitely easier to assess ischemia/infarction with RBBB than with LBBB. This has an anatomic & physiologic basis.
Ken Grauer, MD www.kg-ekgpress.com [email protected]