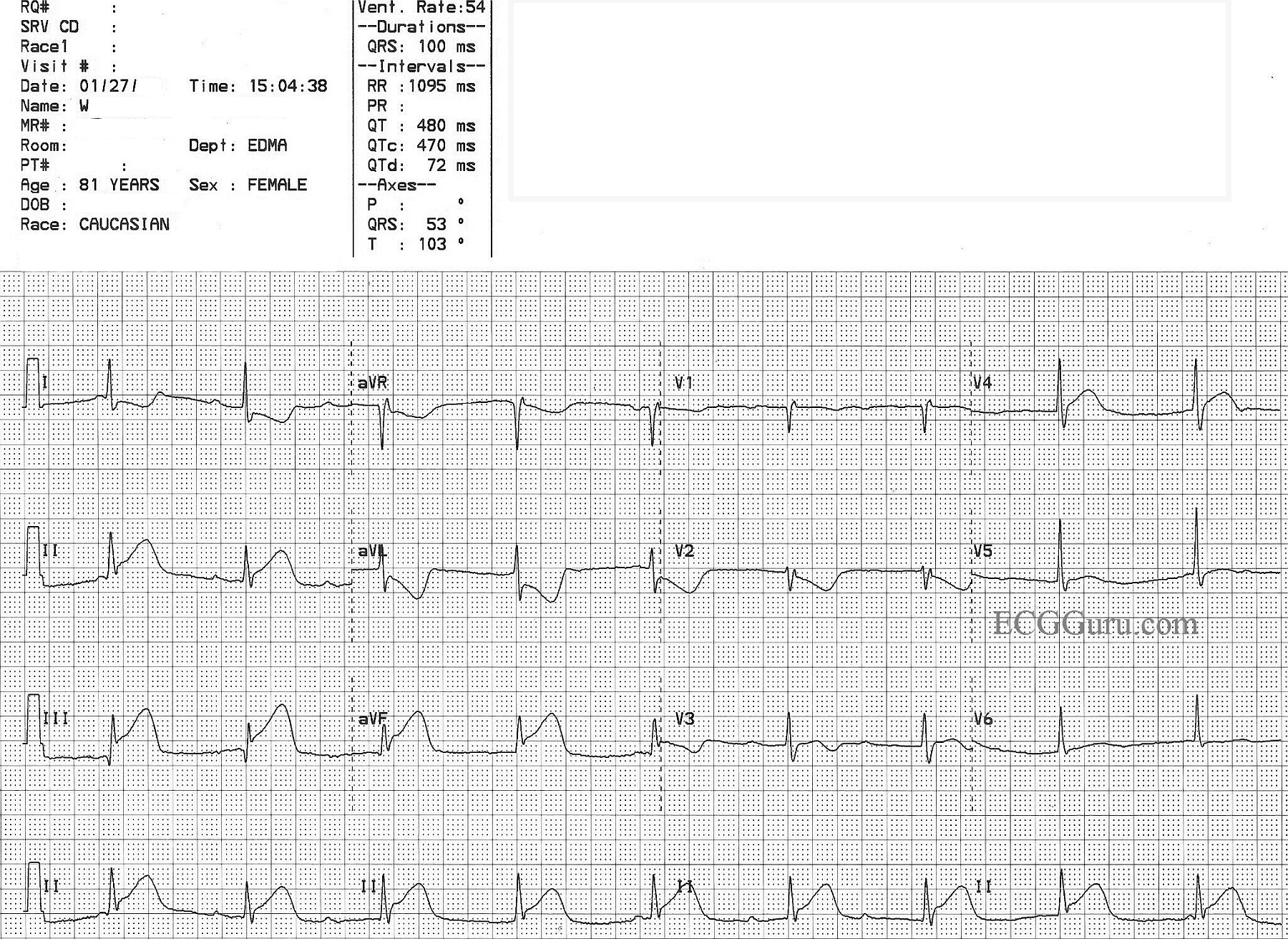
This ECG has always caused a lively conversation in ECG classes, both beginner classes and advanced. There is an obvious underlying sinus tachycardia, with clear P waves.
Some propose that the ECG shows a second-degree AVB, Type II, in that the PR intervals are constant, or nearly so. There is a slight discrepency if you compare the first PRI with the others. The QRS complexes, while very slow, have a pattern of right bundle branch block with left anterior fascicular block - not an unlikely finding in second-degree AV block, Type II, since that is a block in the fascicles of the interventricular conduction system. Type II blocks usually are accompanied by signs of bundle branch dysfunction.
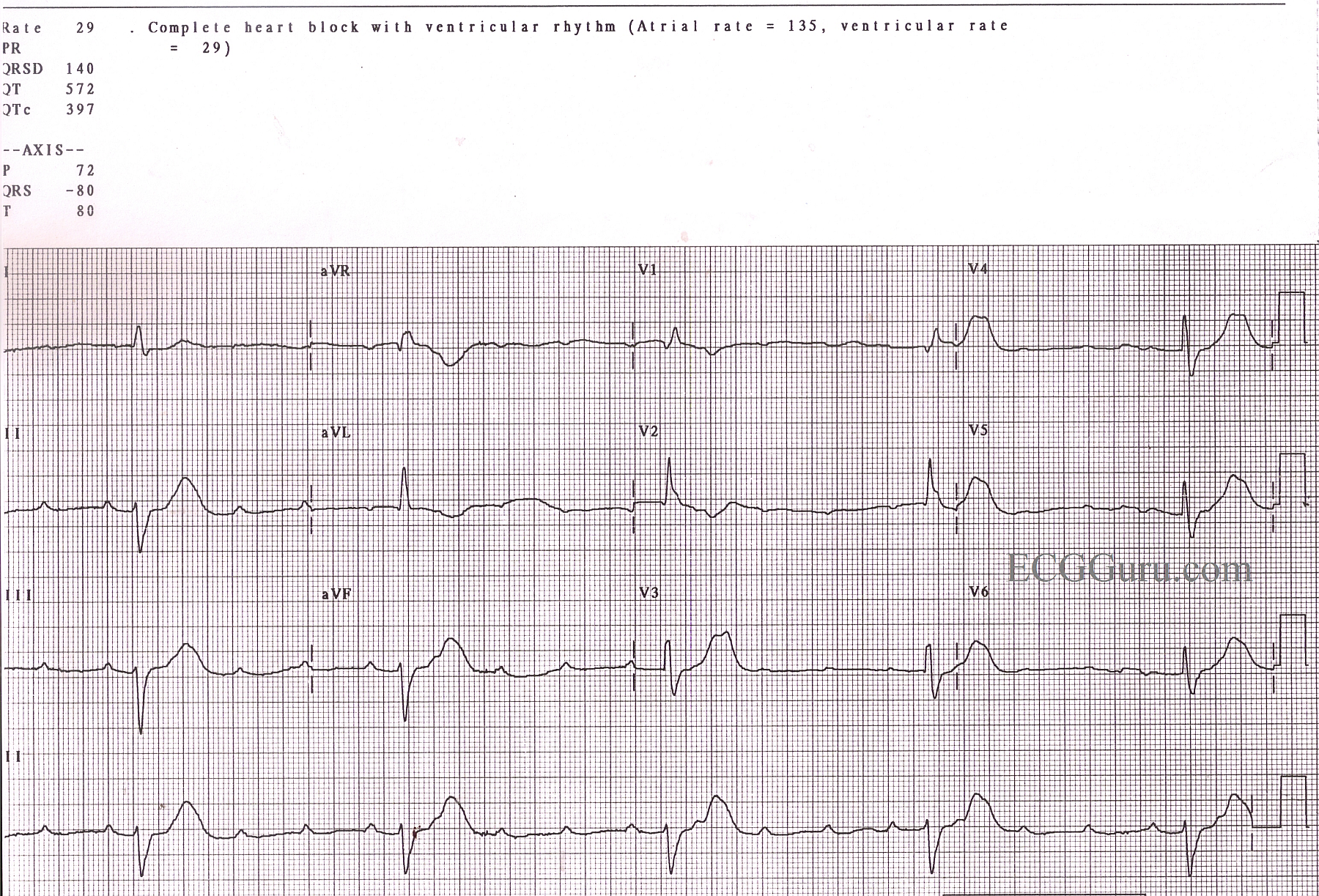
Others strongly believe this is a third-degree, or complete, heart block. They argue that the PR intervals are not identical, and propose that a longer strip would uncover the discrepency. The wide QRS complexes have a strong left axis deviation, which could support the argument for idioventricular escape rhythm.
What do you think? Please comment below.