
Submitted by Dawn on Wed, 04/10/2013 - 22:23
This ECG was donated to the ECG Guru by Dr. Arnel Carmona, one of our favorite Gurus. You will not often see such a great example of this. We are very grateful to Dr. Carmona for his contribution to learning. Dr. Carmona's new blog is EZG - ECG for beginners and enthusiasts.
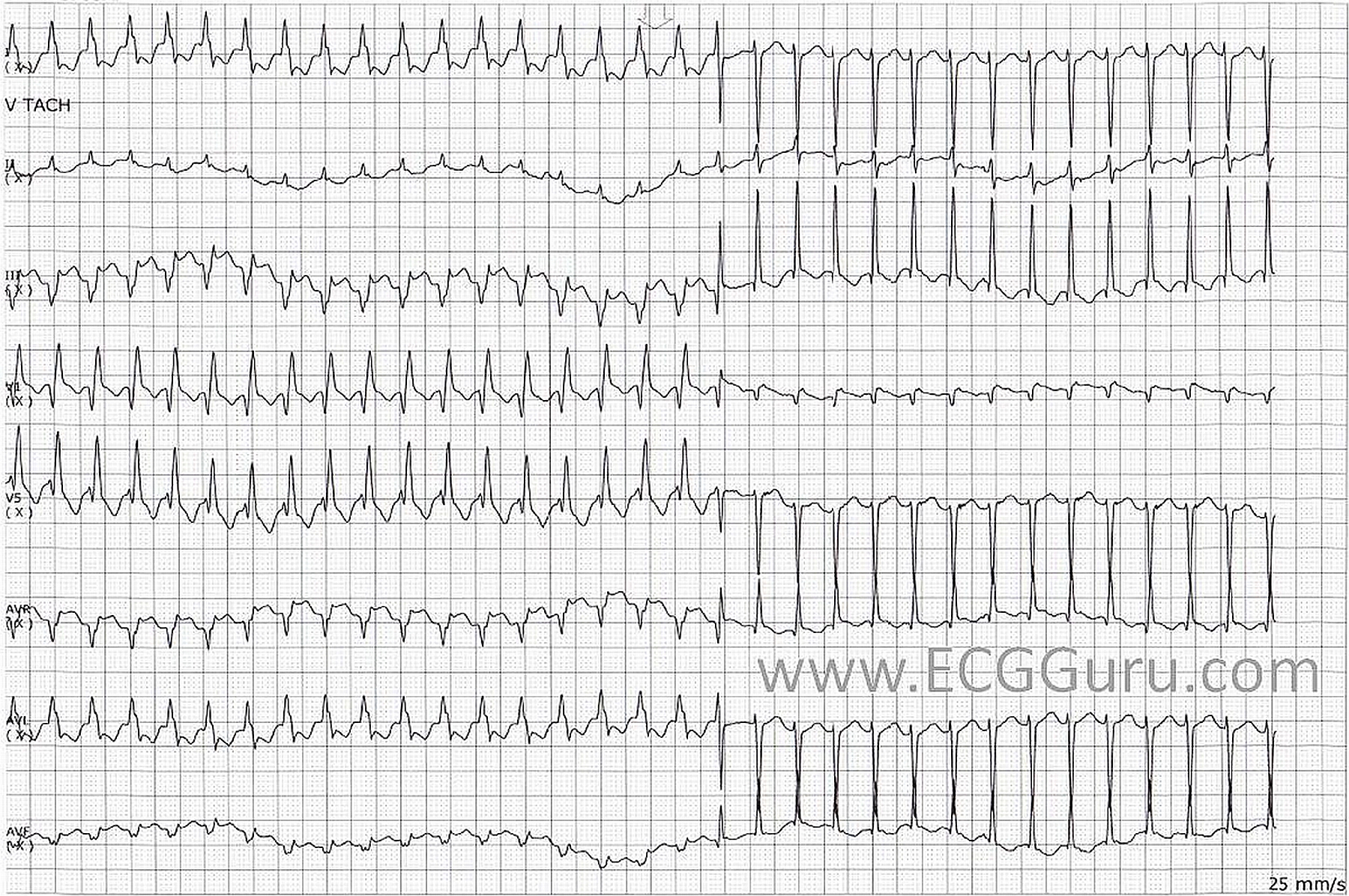
An adult patient was admitted due to palpitations. What is this rhythm?This is a tachyarrhythmia that initially is regular wide complex (RBB morphology) and later became regular narrow complex at a rate of about 187 bpm. There is normalization of the QRS without a change in heart rate. In the latter part of the tracing (narrow complex), pseudo-r can be seen in V1. So, this is SVT with aberrancy with spontaneous normalization.
What is the cause of the intraventricular aberration during acceleration of heart rate? It could be due to failure of the refractory period to shorten or possible lengthening in response to acceleration.
What is the cause of the normalization of the of the QRS? The normalization of intraventricular conduction could be due to the gradual shortening of bundle branch refractory period in response to the tachycardia.
What is the possible mechanism maintaining the aberration? It is likely due to the transeptal concealed conduction blocking conduction in the contralateral bundle. With dissipation of transeptal conduction, the QRS complex normalizes.
What happened to the case? Adenosine was given, terminating the arrhythmia.
Ref:
Fisch C. 1983. Aberration : Seventy-five years after Sir Thomas Lewis. BHJ 50:297-302
Fisch C and Knoebel SB. 2000. Electrocardiography of Clinical Arrhythmia. New York. Futura Publishing Co
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Interesting tracing as always
Interesting tracing as always by Dr. Carmona! Would have been really nice to see a full 12-lead before and after of this patient. From what I see - while lead V1 is consistent with RBBB aberration- lead V5 during the wide-QRS tachy part is not ... so raises the question of what type of aberration ...
Ken Grauer, MD www.kg-ekgpress.com [email protected]
But even the 'normal' QRS isn't normal
The narrow QRS part of the ECG shows a big right axis deviation (+150) with an abnormal morphology in V1 (notwithstanding the pseudo r wave) and a very negative V5. Does this indicate a lesser degree of aberration or is it due to something entirely unrelated? (There's also a nice transitional complex at the end of the broad QRS section.)
Dave R
Patiently Waiting for Follow-Up Tracings to Prove Diagnosis ...
Admittedly - it is difficult to think another reason for transition from wide-to-narrow tachycardia at precisely the same rate other than aberrant conduction with QRS narrowing as aberration resolves. That said:
So - in the aim of fostering academic discussion - I am not at all convinced that this represents aberrant conduction without additional clinical information and more tracings ...
Ken Grauer, MD www.kg-ekgpress.com [email protected]
My 2 cents
I am always suspicious of tracings from telemetry, because the monitor tech often has no control over electrode placement. I wonder if that is a factor is the QRS morphology / axis questions? Even so, it is a very interesting ECG because the two seemingly separate rhythms are so close in rate, and transition cleanly from one to the other, with a transitional or fusion complex between them. If the WCT has a RBBB, does it also have a left anterior fascicular block, bringing the axis to the left? Why is the narrow complex rhythm showing such a severe right axis deviation?
In the WC rhythm, there is a pathological Q in II and aVF, and also in V1. This would lead me to suspect RVMI. Is there significant RV strain? I have questions, not answers, and I am hoping more Gurus out there will comment on this interesting ECG.
Dawn Altman, Admin