
Submitted by Dawn on Mon, 11/04/2013 - 13:40
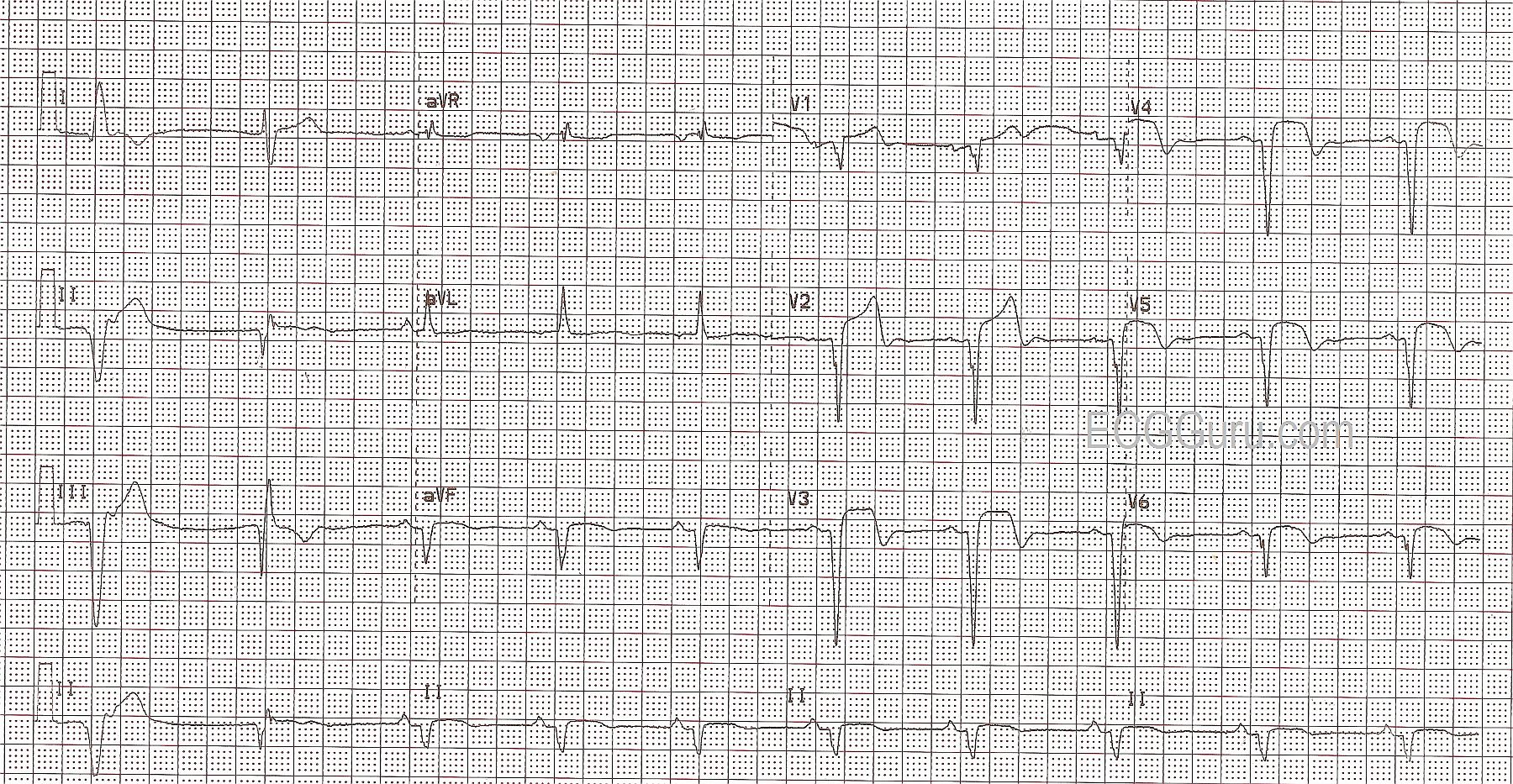
This ECG illustrates an acute anterior wall M.I. in a patient with a previous history of inferior wall M.I. The anterior wall M.I. can be seen in the classic signs in V1 through V6: ST elevations with coved upward shape (tombstones), T waves inverting beginning around V2 and continuing through V6, and pathological Q waves in V1 through V6.
The patient had a history of previous inferior wall M.I., unknown age. This is normally seen in Leads II, III, and aVF. The first two complexes on the strip are wide QRS complexes without associated P waves, presumably ventricular. It is impossible to know from this ECG whether the first complex is a PVC or escape beat, but the second appears to be escape. So, to evaluate the ST segments, T waves, and pathological Q waves in the inferior wall, all we have are aVF and the Lead II rhythm strip at the bottom. These show pathological Q waves (necrosis), and some slight elevation of ST, with coving or horizontal flattening. From this, we know there is damage in the inferior wall, but the age of the M.I. is undetermined.
This patient went to the cath lab, and received angioplasty with stenting of the proximal left anterior descending branch of the left coronary artery.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Anterior Infarction of Uncertain Age ...
Challenging tracing given that we are not given more specifics in the history regarding onset and duration of symptoms.
My interpretation would be ventricular escape and/or ectopy for the first 2 beats - old inferior MI - anterolateral infarction of uncertain age. Probable prior anterior infarction with possible recent and/or acute injury. Urge clinical correlation. If I was working in an emergency department - I'd NEED to know specifics in the history in order to know how to manage this patient. Availability of a prior ECG would be invaluable.
P.S. If I was told that the ECG picture shown here was chronic - one would need to add ventricular aneurysm to the differential. Alas, this patient was taken acutely to the cath lab and underwent reperfusion - so presumably at least a component of the precordial lead abnormalities were acute ...
Ken Grauer, MD www.kg-ekgpress.com [email protected]
No more history available
So sorry that there is no more history available, as this one is from our archives! The patient did have chest pain, uncertain as to the duration of the pain. The LAD was 100% or nearly 100% occluded acutely. The ED physician had much more to go on at the time, but it is lost to history now!
Dawn Altman, Admin