
Submitted by Dawn on Thu, 08/12/2021 - 15:08
This ECG is taken from an elderly man with heart failure.
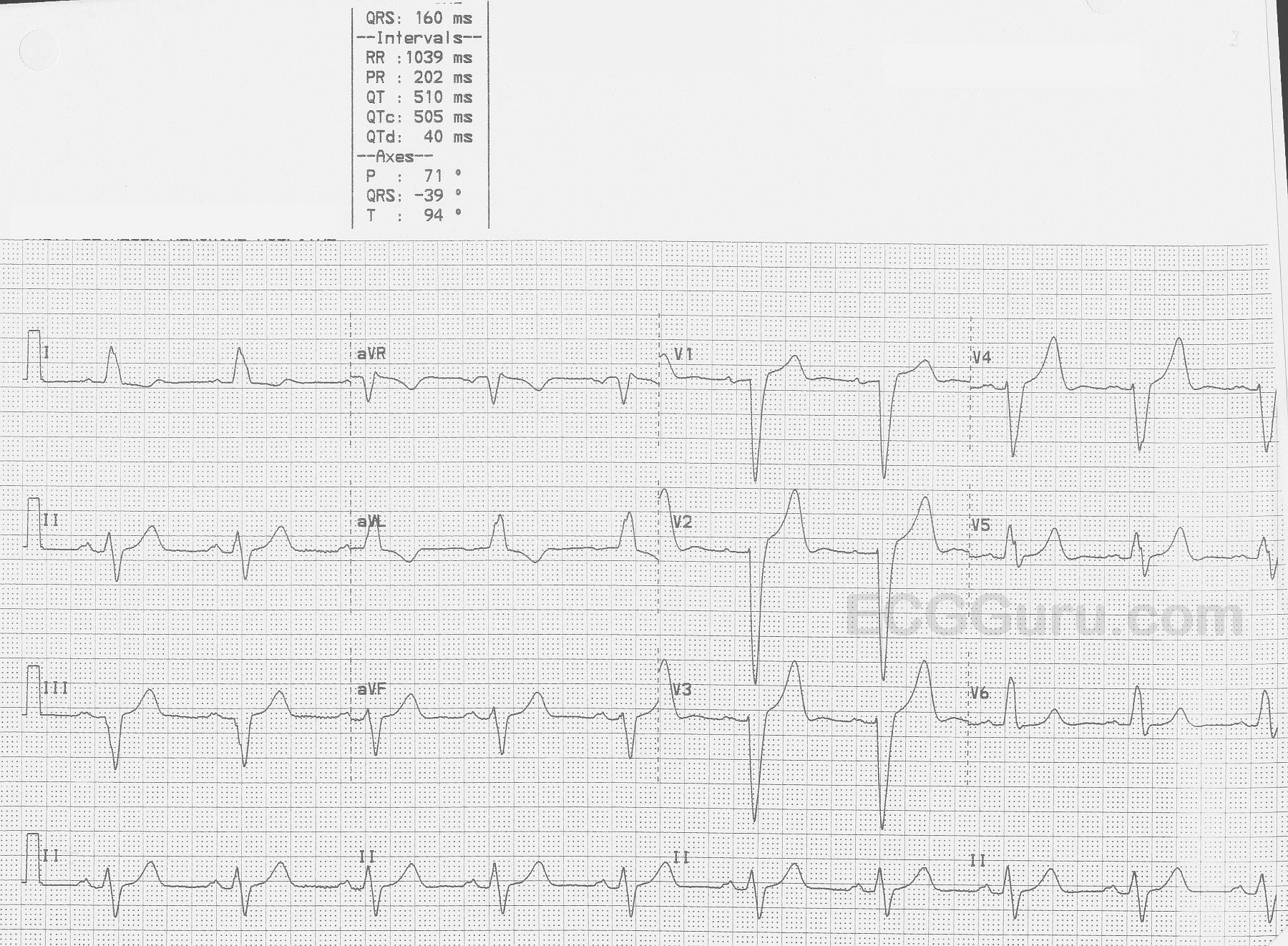
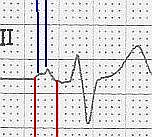
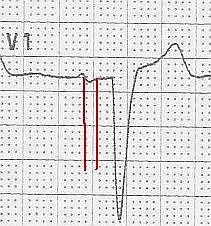
The ECG The first feature that might capture your attention is the wider-than-normal QRS complex, which is 160 ms (.16 seconds). The rate is 58 bpm. We do not know the patient’s medications or baseline rate. There are P waves present, and so the rhythm is SINUS BRADYCARDIA. The P waves are broad , > 110 ms in Lead II (red lines in close up) and bifid, with greater than 40 ms between the two peaks in Lead II (blue lines). In V1, the P waves are biphasic, with the terminal negative portion greater than 40 ms duration (red lines). This meets the ECG criteria for LEFT ATRIAL ENLARGEMENT, or preferably, LEFT ATRIAL ABNORMALITY. (https://LITFL.com/left-atrial-enlargement-ecg-library/) ECG criteria are not highly accurate for detecting atrial enlargement, and abnormal findings should be confirmed by anatomic measurement. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2244611/).
The QRS complexes, as mentioned, are wide. Because there is sinus rhythm, we know the delay in conduction is due to interventricular conduction delay, and not to ventricular rhythm. This ECG meets the criteria for LEFT BUNDLE BRANCH BLOCK.
· Supraventricular rhythm
· Wide QRS (>.12 seconds)
· Upright QRS in Leads I and V6
· Negative QRS in Lead V1.
Both left atrial abnormalities and left bundle branch are associated with heart failure. The leftward axis at -39 degrees is commonly seen with left bundle branch block.
The ST segment elevation in V1 through V4 is normally seen in LBBB. The amount of elevation will be associated with the depth of the negative QRS complex. That is, the deeper the QRS, the higher the STE will be. ST segments and T wave size and shape can be altered by LBBB. If a patient with LBBB has symptoms of acute coronary insufficiency, further evaluation is warranted. On the topic of LBBB and acute M.I., the Smith-Modified Sgarbossa Criteria should be reviewed, as it is one of the most accurate predictors of acute coronary occlusion in the patient with LBBB.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.