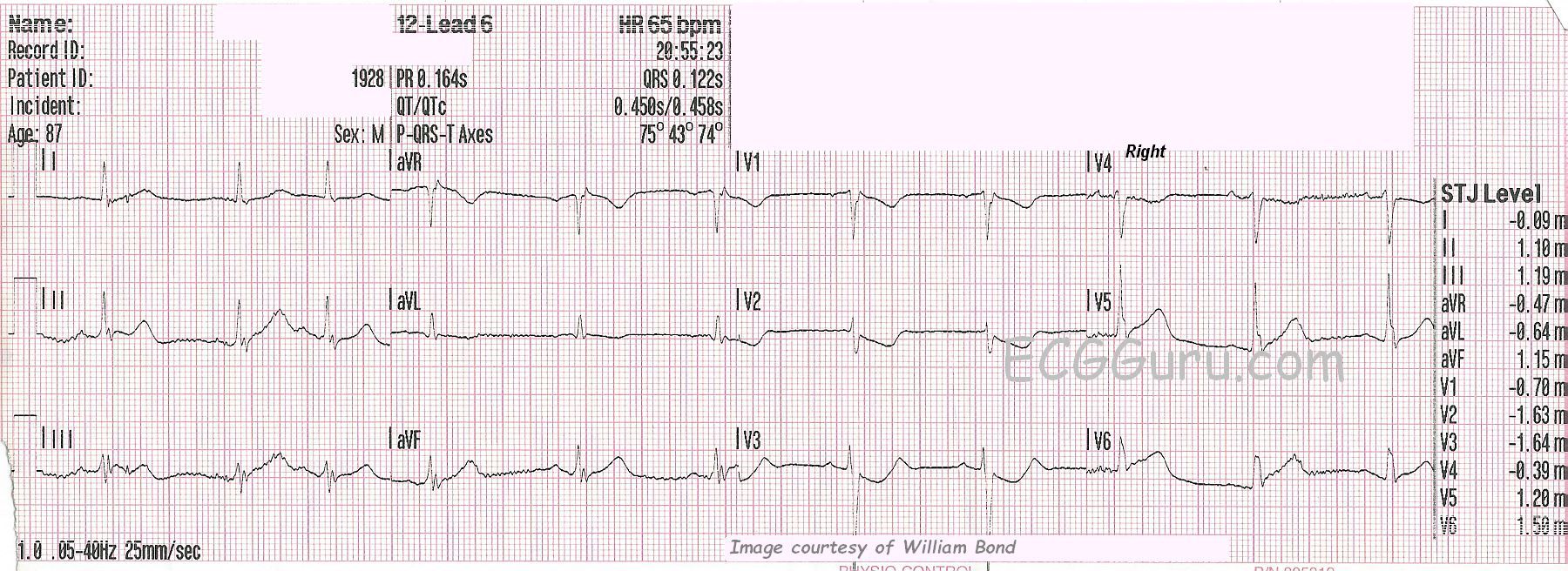
SUBTLE ST CHANGES This ECG was obtained from an 87-year-old man who was experiencing chest pain. Due to the subtle ST elevation in Leads II, III, aVF, V5, and V6, (inferior- lateral walls) the ECG was transmitted to the hospital by the EMS crew, and the cath lab was activated. The patient denied previous cardiac history.
In addition to the subtle ST elevation, there is ST depression in V1 through V4, which represents a reciprocal view of the injury in the inferior-posterior-lateral wall. Because the anterior wall is superior in its position in the chest, it is opposite the inferior/posterior wall, and can show ST depression when the inferior-posterior area has ST elevation. This ECG was the 6th one done during this EMS call. Prior to this one, the ST segments were elevated less than 1 mm. This is a good example of the value of repeat ECGs during an acute event.
RIGHT VENTRICULAR M.I.? This ECG was done with V4 placed on the right side, to check for right ventricular M.I., which is a protocol for this EMS agency. When the right coronary artery is the culprit artery (about 80% of IWMIs), RVMI is likely. In RVMI, we would usually see reciprocal ST depression in Leads I and aVL, but the STE is very subtle here, so the depression would likely be also. When the culprit artery is the left circumflex artery (<20%), lateral lead ST elevation is more likely, as we see here in V5 and V6.
WHAT ABOUT RHYTHM? The rhythm is sinus with PACs. PACs are considered to be benign in most situations, but in a patient with acute M.I., any dysrhythmia can be concerning. The QT interval, measured as QTc (corrected to a heart rate of 60 bpm), is slightly prolonged at .458 seconds (458 ms). Over .440 seconds is considered prolonged in men, and over .500 sec. places the patient at increased risk of developing torsades de pointes. CAD and myocardial ischemia can lead to this modest increase in QTc.