
Submitted by Dawn on Thu, 02/07/2013 - 23:00
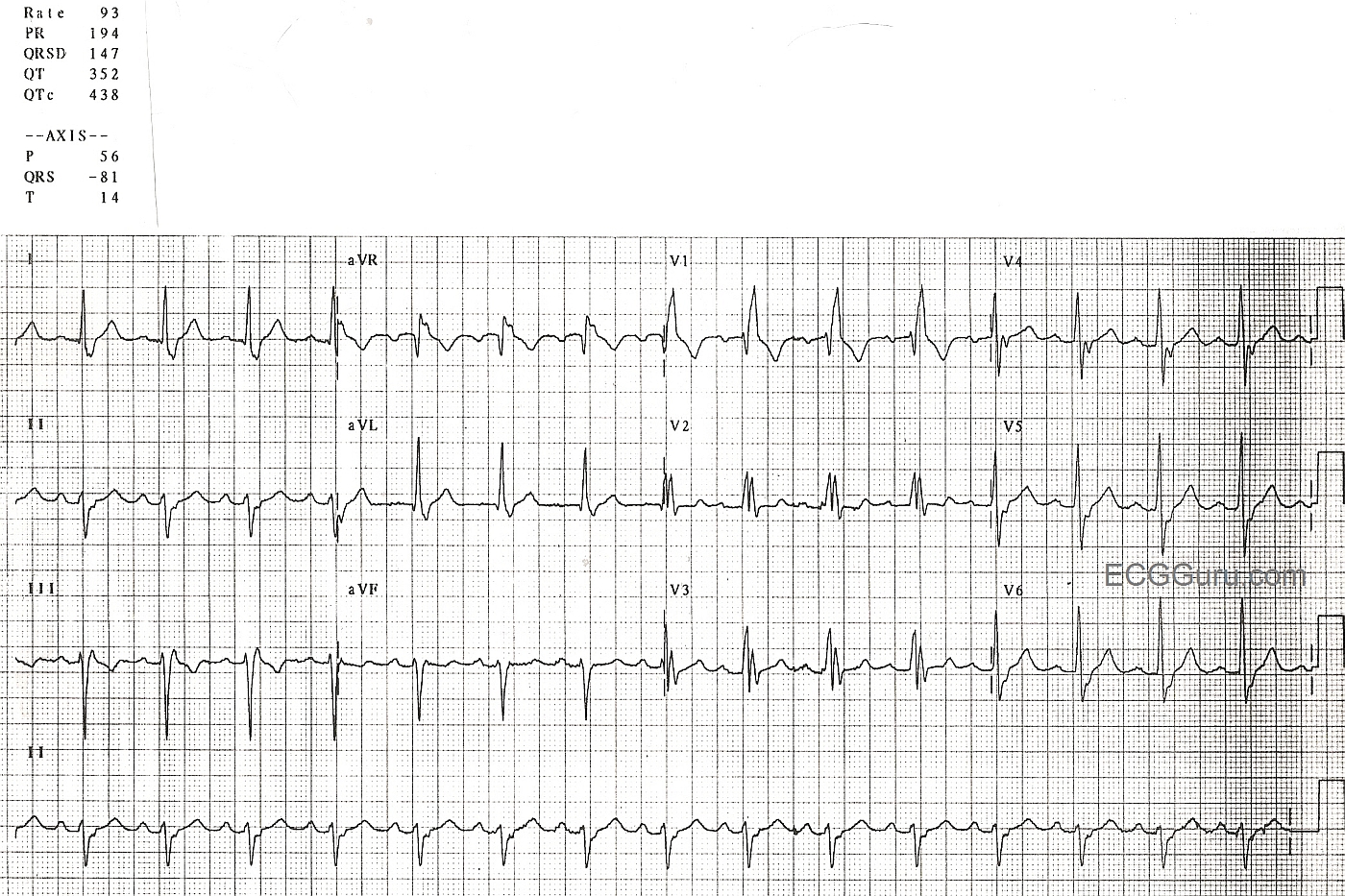
This is a nice, clear right bundle branch block pattern: wide QRS, supraventricular rhythm (NSR), and rSR' pattern in V1. Wide little s waves in Leads I and V6 are also diagnostic. The left axis deviation indicates a left anterior fascicular block, since there is no other apparent reason for the left axis deviation, such as pathological Q waves or LVH. Left anterior fascicular block is a diagnosis of exclusion, also considering that RBBB and LAFB are often seen together (bifascicular block), since the two fascicles have the same blood supply.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Nice RBBB/LAHB
Nice example of bifascicular block with RBBB/LAHB. No acute changes are seen. There may be LVH. The criterion for satisfying LVH in lead aVL is an R wave amplitude of at least 12 mm. It is interesting to note how R wave amplitude changes for the 3 beats recorded in lead aVL. This voltage criterion is satisfied for the first 2 complexes in lead aVL - but not the 3rd one. Although I'd still note, "probable LVH" - it is well to remember that the specificity of this criterion is decreased in the presence of LAHB since the sequence of depolarization (and therefore QRS amplitude) is altered with LAHB.
Ken Grauer, MD www.kg-ekgpress.com [email protected]
LAHB
If you could clearly diagnose the LVH in this ECG, would you then not be able to diagnose the LAHB from the axis deviation?