
Submitted by jer5150 on Sat, 04/06/2013 - 12:18
At this time of posting, I currently have no clinical data for this patient. This ECG is of interest because of its arrhythmic and nonarrhythmic elements.
I can think of at least two possible explanations for the mechanism of this rhythm and both would benefit from being illustrated by a laddergram.
One mechanism is rather exotic and has not been previously seen here on this website or discussed in the various FB forums.
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
My stab at it
Without actually mapping anything out and just eyeballing things here is my first guess. I'm not sure the exact "proper" way of saying this so I'll write it out very wordy.
This appears to be a junctional rhythm with retrograde conduction to the atria. Of interest, there seems to also be a 2nd degree AVB Type 1 as evidenced by the retrograde P wave that is in the ST/T area at the beginning of the tracing then before the QRS at the 4th complex. The 3rd QRS complex appears to be associated with the retrograde P wave so is it possible that this person on top of everything else has an accessory pathway that was no able to conduct? If so this person was very close to developing an antidromic re-entry rhythm!
Am I totally off base here?
Oh, and there is an inferior STEMI apparently which is probably the trigger of all the stuff above.
Just thinking it through more
Just thinking it through more, if my above interpretation is so then the person would not develop a re-entry rhythm as the AVB would prevent that (or at least not let it last long).
Exotic Atrial & Junctional Escape with Acute inf-post-lat MI
Highly interesting tracing. Initially I was considering retrograde conduction in the first 3 T waves (no QRS for that first T wave) - with progressively longer R-P intervals - until an echo beat occurred (3rd QRS on the tracing - conducts with some RBBB aberration).
Then I took out calipers and was surprisingly able to march out quite regular negative P waves in lead II at a rate ~34/minute - so rather than retrograde conduction - I'm inclined to think that there is in fact a very slow atrial rate. This P wave is of small amplitude - and looks to be negative in lead II, ergo NOT a sinus rhythm - but rather a very slow ectopic atrial focus. There is a slightly faster (~36/minute) junctional escape rate - with AV dissociation between these two escape foci. The negative P wave in the T of the 2nd QRS occurs late enough such that it DOES conduct - albeit with RBBB aberration. The last 3 QRS complexes on the tracing represent that junctional escape rhythm (with AV dissociation by default from the even slower ectopic atrial focus).
QRS morphology from these junctional beats suggests acute infero-postero-lateral MI.
I'll look forward to Jason's revealing laddergrams.
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Difficult to choose
Two great explanations from Ken. I had a go at this before reading Ken's submission and I came up with his first suggestion, of a junctional escape rhythm with retrograde Wenckebach-type conduction pattern ending in an echo beat. Of the two explanations I prefer this one but only, I think, because I find it a more attractive idea! I'm looking forward to finding out whether Jason will come up with yet another possible explanation.
Dave R
INTERPRETATION
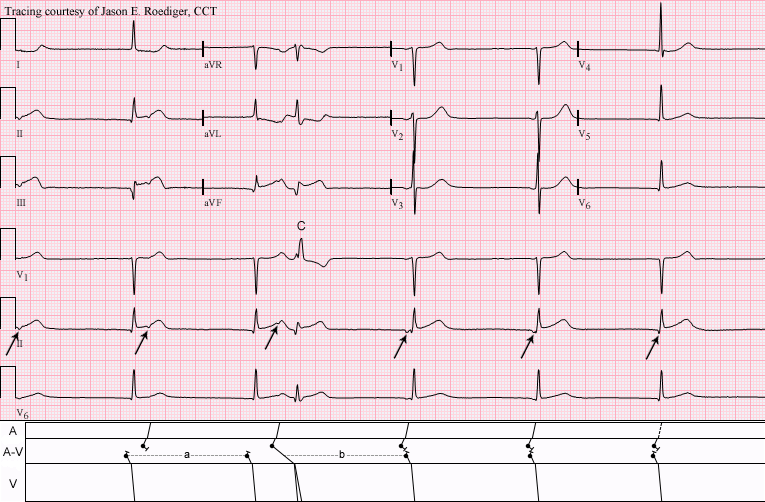
INTERPRETATION:A-V dissociation between an upper-level junctional escape pacemaker (rate 37/min) from a lower-level junctional escape pacemaker at a slightly slower rate of 35/min, with ventricular capture (3rd beat) by the higher pacemaker; the capture beat (C) is conducted with RBBB aberrancy (see laddergram). There is also an associated acute inferior infarction.
COMMENTS:
Note that the P’-P’ intervals are constant which establishes the interpretation of two independent junctional pacemakers rather than a junctional escape rhythm with reciprocal beating. Also note in the A-V tier that cycle "a" is exactly equal to cycle "b". An equally plausible interpretation is the presence of an ectopic atrial bradycardia dissociated from an idiojunctional escape rhythm (not diagrammed here).
SOURCE / REFERENCE:
(1.) Marriott HJL. Pearls & Pitfalls in Electrocardiography. 1st ed. Baltimore: Williams & Wilkins, 1998, p 66-67
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]