
Submitted by Dawn on Mon, 10/05/2015 - 17:26
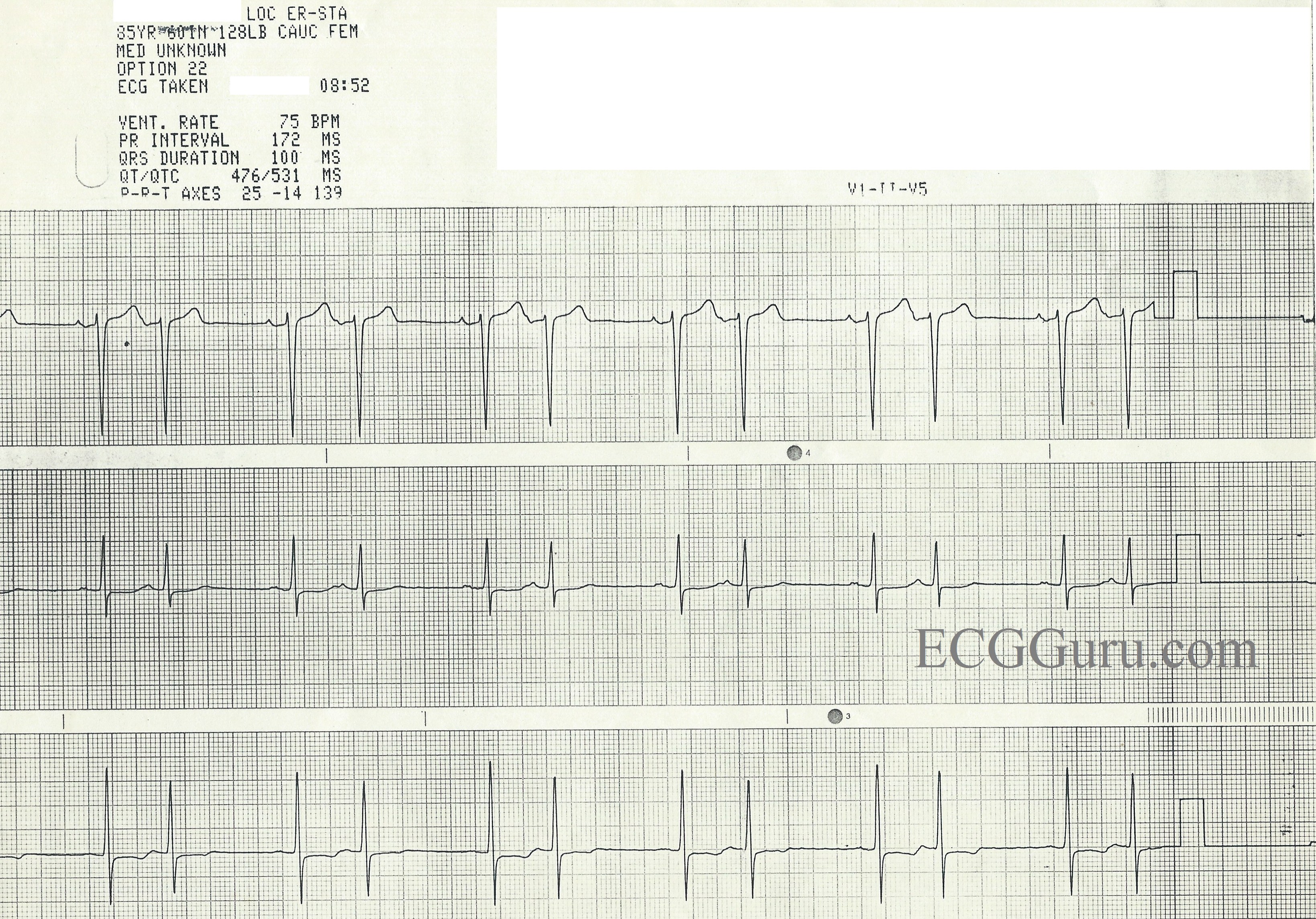
This three-lead rhythm strip is from an 85 year-old-woman for whom we have no other information, unfortunately. It shows an obvious, regular bigeminal pattern. There are many rhythms that can cause bigeminy, with regular, paired beats. So, how do we analyze this rhythm?
First, we can see that all the QRS complexes are fairly narrow and look alike in each lead. So, we know this is a supraventricular rhythm. The rhythm “marches out”, with the same spacing between all the paired beats, and exactly one P-QRS missing after each pair.
Sino-atrial exit block occurs when the sinus node fires, but the impulse is unable to exit the sinus node. No P wave will occur, but the sinus node continues to fire in a regular rhythm. There are four types of SA block, just as there are four types of AV block. This ECG meets the criteria for a Second-degree, Type II SA block.
First-degree SA block would not be decipherable on the ECG, as we do not see the SA node fire, and therefore cannot measure an interval between the SA node firing and the production of a P wave.
Second-degree SA block, Type I would have progressively prolonging exit times for the impulse leaving the SA node. This would produce progressively shortening R-to-R intervals, until the pause.
Second-degree SA block, Type II has regular R-to-R intervals until the pause, and the pause will equal two or more (usually two) R-to-R intervals.
Third-degree SA block produces NO P WAVES, and would have to be diagnosed on electrophysiology studies, as it would usually result in a junctional escape rhythm.
Differential diagnosis includes many causes of “atrial bigeminy”. When every other beat is a premature atrial contraction (APB or PAC), the pause will be caused by the PAC “re-setting” the sinus node, and will not be a multiple of the R-to-R interval on that strip. We can differentiate this rhythm from the AV blocks because in sinus block, the P wave is missing. In AV block, the P wave is present, but not always conducted.
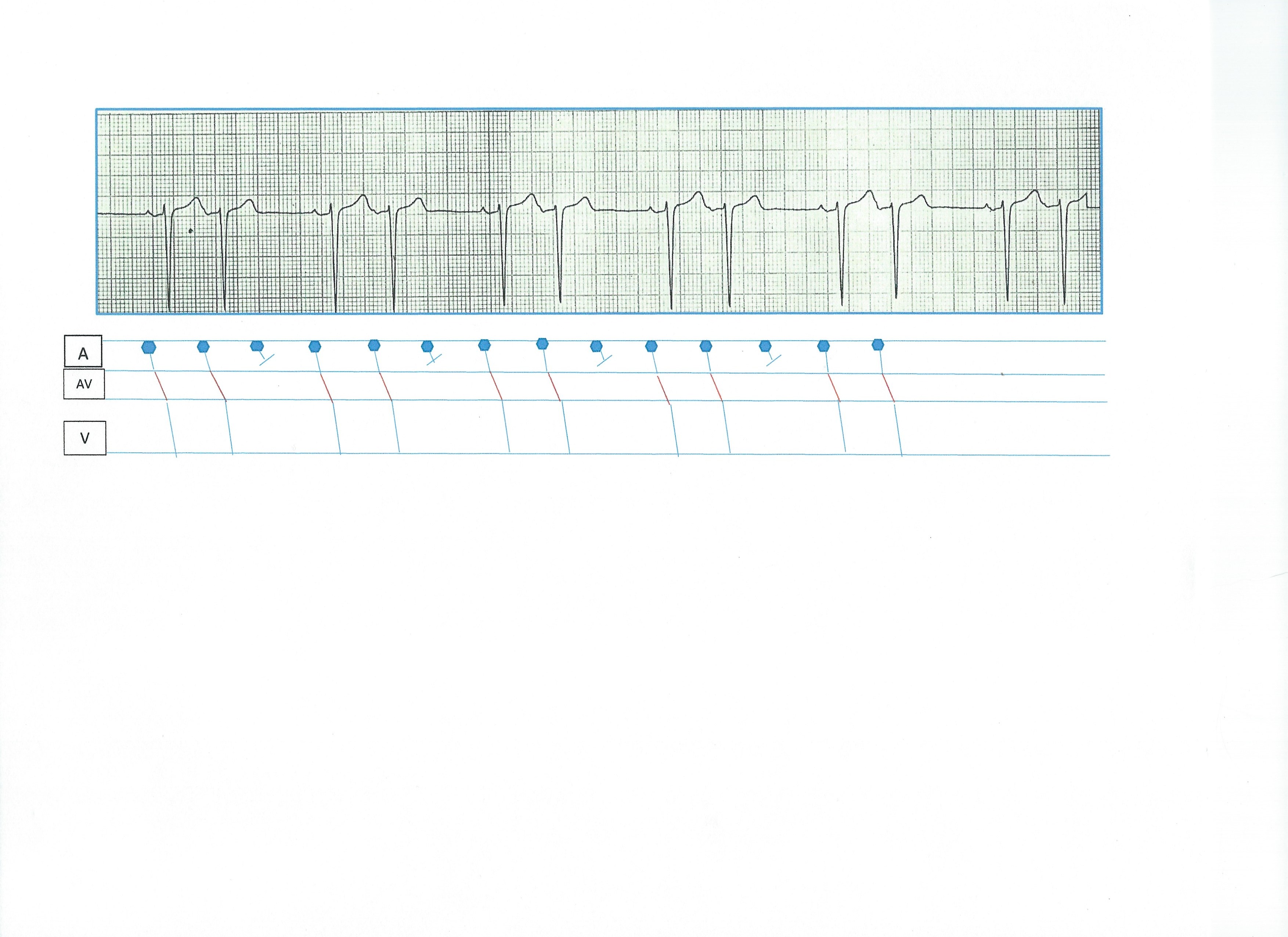
To better illustrate what may be happening in this ECG, we have included a laddergram. If you are not familiar with using laddergrams, please refer to the following links.
ECG Guru, Are You New To Laddergrams, Dr. Ken Grauer, Making A Laddergram.
Clinically, we would want to investigate the possible cause of the SA block or atrial bigeminy, and watch for worsening of any block, which could result in a dangerous bradycardia.
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
SA Block — or Maybe Not?
One of the most difficult diagnoses to make (in my experience) — entails recognition of Type I and Type II SA block. Reasons for this difficulty include: i) SA Block is NOT common. In my experience, most of the time when the rhythm is thought to reflect SA block — it often turns out to be something else …; ii) We do NOT (by definition) see a P wave in front of the dropped beat. Therefore, we have to postulate the presence of a P wave that isn’t there in front of our eyes (but rather never made it out of the SA node); iii) It is often VERY difficult to be certain IF P wave morphology of the P waves that we do see is identical (as it must be, if we are dealing with SA block rather than intermittent PACs); and iv) The timing of QRS complexes is often not as the textbook says it is (due either to underlying and unpredictable sinus arrhythmia — and/or due to SA block variations that are not strictly of the Mobitz I or Mobitz II type … ).
That said — SA block DOES exist — and, as it does imply a potential problem with the conduction system (depending on the associated clinical scenario) — it is well to be aware of how and when to recognize it.
I suspect the example here is not SA block because: i) it looks like P wave morphology is different for each early-occurring beat compared to the P wave morphology preceding beats that end after the longer R-R interval; ii) When measured with calipers — I think the timing is off … (ie, coupling intervals vary; depending on where one measures the peak of the P wave — I don’t think we always get double the P-P for duration of the pause … ); iii) If the rhythm was Sinus with SA block — then the atrial rate would be ~115/minute, and that would be a fairly rapid rate unless there was some provocation; and iv) Atrial bigeminy is far more common than SA block is …
Clinically — MUCH more important than whether this is or is not SA block — would be what is going on with the patient. SA block may at times be relatively benign in an otherwise healthy patient without other evidence of conduction system disease. On the other hand, it may represent one more manifestation of a severe conduction disorder in a patient with other prominent problems.
Diagnostically — MUCH more important (in my opinion) than whether this is or is not SA block — is to recognize the above reservations that I present — AND — to be aware that “proof” that this is (or is not) SA block would require additional monitoring until such time that we could be comfortable that: i) ALL P waves are indeed of identical sinus morphology; ii) That there is no underlying sinus arrhythmia (because coupling intervals in this example are not constant … which would suggest either PACs or underlying sinus arrhythmia ); iii) That the patient was not having sinus tachycardia (if this is SA block, then the atrial rate is ~115/minute ...); and iv) The patient is not having definite evidence of PACs … (Despite my suspicion — I admittedly cannot be 100% certain that the early beats here are PACs ... ).
BOTTOM LINE: There is often more than 1 possible explanation to interesting arrhythmias. I would interpret this example as probable Atrial Bigeminy. By way of perspective — I recall a fair number of tracings over my 35+ year career in which I would be left with at least some indecision as to whether a tracing represented Atrial Bigeminy or a form of SA Block.
P.S. SA Block might best be illustrated on laddergram by adding an additional Tier to the diagram (ie, an SA Nodal Tier). I illustrate this in brief review on the SA blocks (excerpted from my ACLS-2013-ePub) — CLICK HERE to DOWNLOAD —
Ken Grauer, MD www.kg-ekgpress.com [email protected]
This is a difficult one, Dawn!
Wow! I think the greatest thing to learn from this ECG is that you can't always be 100% sure what the diagnosis is - no matter how advanced your knowledge or skill. Some arguments just can't be settled with a 12-lead ECG.
Our patient is 85 y/o and we really know nothing of her general health status. Yes it IS possible that this is a 2nd degree SA block, but could it also be an atrial bigeminy? If this were an atrial bigeminy, the ectopic atrial depolarization will either reset the SA nodal pacemaker resulting in a non-compensatory pause or the SA node will be protected by an entrance block resulting in a compensatory pause.
Let's assume that this is an atrial bigeminal rhythm and the atrial ectopic beat invades the SA node and resets the SA nodal pacemaker with each rhythm. The sinus P wave that follows the second beat of each couplet will terminate a sinus P - P interval after having been reset by the atrial ectopic beat. How wide is this P - P interval? Well, we really can't be sure because sometimes the discharge and resetting of the SA nodal pacemaker is virtually instantaneous and other times there is a bit of delay before the SA pacemaker resumes firing (we call this "stunning"). In either case, the P - P interval would have to be between either 0.24 - 0.44 second or 0.60 - 1.00 second for the sinus P wave to be visible. This would allow for the P wave to be seen in either the ST segment or the following TP segment. I think it is evident that there is no P wave hiding in the T wave of the second beat of each couplet because is it smaller than the T wave that follows the first of each couplet and which definitely contains a P wave. But we really see no evidence of any P wave after the early atrial discharge until the sinus P that follows at some distance. Does the first P wave of each couplet represent the new, reset P-P interval? Possibly - but we can't know for sure.
Could the rhythm represent atrial bigeminy with a protected SA nodal pacemaker and compensatory pauses? Absolutely! You can't see the sinus P wave following the second beat of each couplet because it would be buried in each QRS.
Again, could this be a 2nd degree SA nodal block? Yes it could. One would have to assume a sinus rate of around 110. However, the patient is 85 y/o and in who knows what kind of health, so a sinus tachycardia and a 2nd degree SA block is totally possible.
However, an atrial bigeminy with compensatory pauses (and make no mistake: atrial premature complexes with COMPENSATORY pauses are NOT rare at all, though many instructors give that impression) is also quite possible and - as Dr. Grauer pointed out - probably more likely statistically.
Whether this is an atrial bigeminy with resetting of the SA nodal pacemaker cannot be reliably determined from these strips.
A question for the novice-to-intermediate students of electrocardiography: What is the most important factor that determines the severity and urgency of a dysrhythmia? Answer: the patient's blood pressure! Never forget that the clinical status of the patient comes first! As regards the actual ECG, the possible presence of any AV block of Mobitz II or greater is the next most important factor. Some might say the ventricular rate is the next most important factor, but I would refer them back to the blood pressure. It doesn't matter what the rhythm is if there is adequate blood pressure and the patient is not in any significant distress. Treat the patient - not the rhythm strip!
Did anyone note the aberrancy of the second beat of each couplet? I assume that the top strip is probably V1. The subtle reduction in the amplitude of the S wave of each early beat indicates a slight slowing of conduction in the right bundle branch.
Jerry W. Jones MD FACEP FAAEM
https://www.medicusofhouston.com
Twitter: @jwjmd
Thank You Dr. Jones!
We greatly appreciate your detailed comment Dr. Jones! As Rosenbaum once said, "Every self-respecting arrhythmia has at least 3 possible interpretations".
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Thank you both
What a great conversation! I agree that atrial bigeminy is more common than SA block. I wanted to put an example of SA block into the archives, and I all I had was this one, given to me by a physician years ago as an example of second-degree SA block. It does meet the ECG criteria, and I am not sure what other evidence might have been present for the diagnosis. I suspect there was a preceding sinus rhythm of 110/min, but I have not been able to locate it in the depths of my files.
I totally agree that the PATIENT is more important than the rhythm strip, and that perfusion status (BP, skin color and temp, mentation) is paramount!
Because of your thought-provoking comments, I am amending the title of this post to indicate that SA block is a possible diagnosis. Thank you, both, Drs. Grauer and Jones.
Dawn Altman, Admin
Second degree SA Block Type II
Here is an example of second degree SA Block Type II from a holter-ecg. I think there is no doubt that it is a real one.