
Submitted by Dawn on Sat, 06/04/2016 - 14:02
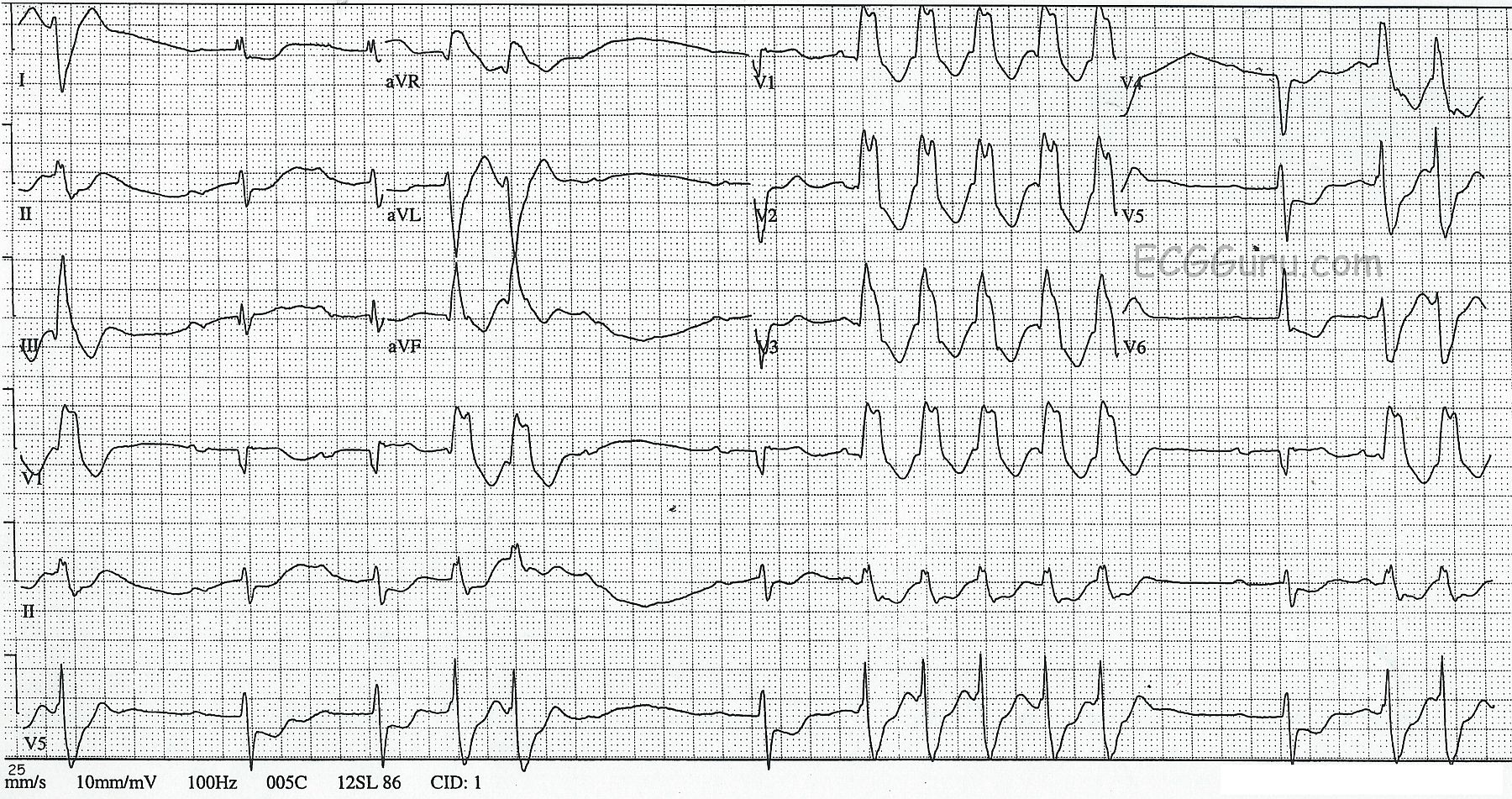
This ECG was obtained from a 45-year-old man who was experiencing palpitations and lightheadedness, which he originally attributed to anxiety. There are short, but frequent periods of ventricular tachycardia, which are self-limiting. This is called "NON-SUSTAINED VENTRICULAR TACHYCARDIA". The underlying rhythm is sinus, with a remarkably long PR interval, and at least one episode of failure of the P wave to conduct, making "second-degree AV block, Type II" a possibility. It is difficult to thoroughly evaluate the underlying rhythm because it is not seen very often in this ECG. The rate of the underlying P waves is about 67 bpm. The PR interval is .40 seconds (400 ms). The "normal" QRS complexes are slightly widened, at about .10 sec (100 ms), which is typical of Type II AVB. The ventricular QRS complexes are wide at .16 sec. (160 ms)
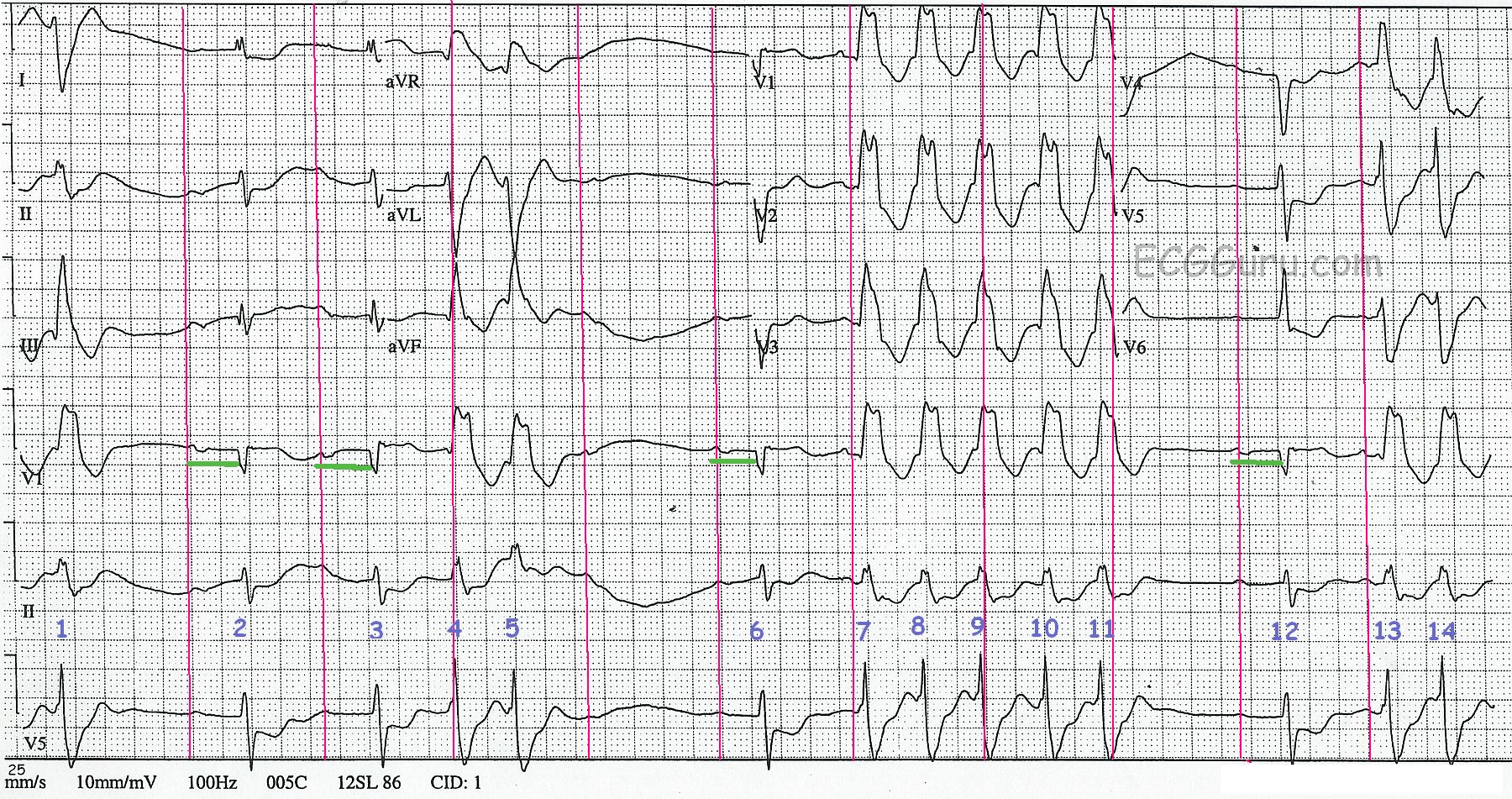
To assist you in using this tracing for teaching, we have also supplied a "marked up" version. The P waves, both visible and hidden, are marked with red lines. The PR intervals are shown in the Lead V1 rhythm strip in green. And the QRS complexes are numbered. QRS complexes numbered 2, 3, 6, and 12 are sinus. The P wave AFTER QRS #5 is non-conducted.
To review the differentiation of ventricular tachycardia from supraventricular tachycardia with aberrant conduction, go HERE.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
A 42yo with NSVT and a Long PR interval
Interesting tracing presented by Dawn — that we unfortunately have no more than minimal history for. There are obvious problems, though precise diagnosis would require additional monitoring than what we have here.
As noted, there are only 4 “narrow”beats (#2,3, 6 and 12). Adding to the difficulty in interpretation is the wandering baseline and tiny amplitude for P waves. I agree that it DOES look like these 4 beats are conducted. I am not as certain that the PR interval is the same for these 4 complexes (the PR interval looks shorter to me preceding beats #6 and 12 than it does for the PR interval preceding beats #2 and 3 … ). I am also not sure the P wave following beat #5 truly had “full chance” to conduct — as it probably encountered some retrograde conduction from the preceding ventricular beat ( = beat #5). So while obvious that this patient has some conduction problems (at best, a prolonged PR interval — some relatively prolonged post-ectopic pauses — and perhaps some 2nd-Degree AV Block) — I’m not sure we can hone in on the specific type of conduction block. My hunch is that this is not Mobitz Type II because: i) the QRS is not overly wide (as it usually is with Mobitz II); ii) I don’t think the PR interval is constant preceding all conducted beats; iii) Mobitz II more often is associated with a relatively normal PR interval, rather than the marked prolongation we see here; and, iv) Mobitz I is so much more common than Mobitz II.
Before focusing on the wide nonconducted complexes — it is worth a look at QRST morphology for those beats that are conducted. There are no conducted beats in leads aVR, aVL and aVF — so we are reduced to 9 leads that allow scrutiny. QRS amplitude of conducted beats is relatively small (especially in limb leads I,II,III). There is a Q wave in lead III. There are QS complexes in V1-thru-V4. The QT interval appears fairly normal (I see the QT best in V5,V6). There is marked ST depression in leads I, II, and V4,V5,V6. There appears to be slight ST elevation in lead V1. This all suggests that this 45-year old man has had prior anterior infarction and manifests ischemic ST-T waves in multiple leads — so there appears to be a “substrate” for the wide rhythm.
As per Dawn — we see a series of wide beats that are clearly ventricular in etiology. The P wave preceding beat #7 appears to be on time — yet long before this P wave can conduct comes a run of 5 wide beats in a row. So this on-time P wave preceding beat #7 represents transient “AV dissociation” — which of itself virtually proves that what follows must be ventricular in etiology. Of note, QRS duration of the wide beats we see is markedly prolonged (at least 0.16 second) — which of itself suggests severe underlying disease. QRS morphology of the wide beats is not typical for any known conduction block — so it is almost certainly ventricular in etiology. We see a single ventricular beat at the onset of the tracing (beat #1) — 2 ventricular couplets (beats #4,5; and #13,14) — and a 5-beat run of NSVT = non-sustained ventricular tachycardia (beats #7-11) at a rate of ~ 140-150/minute.
Bottom Line — It is easy to understand why this 45-year old man presented with palpitations and lightheadedness, which are clearly not due to “anxiety”. He undoubtedly has significant underlying heart disease — with need for cardiac catheterization to define his anatomy.
NOTE: For additional review on assessment of Wide Tachycardias — Please check out my ECG Blog #42 —
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Great Teaching ECG!
Great ECG, Dawn! A lot to be learned here. This ECG looks horrible (which is good for anyone learning ECGs because THIS is what usually shows up on your chart at 3 am in the morning when the cardiologist on-call has just gotten home from spending four straight hours in the cath lab)!
The first thing that you must remember is that you approach an ECG like this one just as you would approach one that is seemingly normal - in a regular, methodical manner.
The basline rhythm is sinus and appears very regular. Dawn indicates the rate is 67/min and that certainly appears correct. There is an underlying first degree AV block. When I measure the PR intervals with my calipers, I see that the 6th P-QRS complex has a PR interval that is definitely shorter than the others (I think the PR interval of the 12th P-QRS is basically the same as the 2nd and 3rd PR intervals). There also appears to be a baseline left axis deviation.
I would agree that the P wave following the 5th QRS complex was blocked due to interference in the AV node and is not a true Type II AV block. I feel that the 6th QRS complex is a junctional escape beat in that it appears a bit too early to be related to the preceding P wave (this is the beat with the shorter PR interval), it has a QRS morphology just like the sinus conducted beats and, most importantly, it terminates the longest R-R interval on the tracing.
The wide complexes are most certainly short runs of ventricular tachycardia at a rate of about 150/minute - a very typical rate for V-tach. The ectopic focus is high up in the left ventricle based on the morphology of the ectopic QRS complexes in V1 and most likely originating somewhere in the distribution of the left anterior fascicle. The predominantly positive ectopic complexes in the inferior leads (with an LPFB morphology) indicate impulses traveling toward the inferior leads. As Dr. Grauer pointed out, the presence of the underlying ischemic ST segments certainly indicates the typical substrate for a ventricular tachycardia.
Thanks again, Dawn, for a challenging ECG and a great website!
Jerry W. Jones MD FACEP FAAEM
https://www.medicusofhouston.com
Twitter: @jwjmd