
Submitted by jer5150 on Sat, 10/27/2012 - 12:41
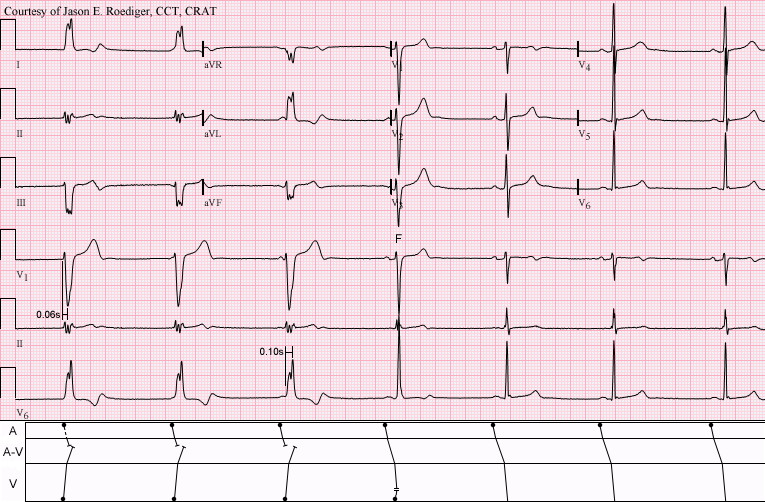
This is one of five consecutive serial ECGs that I performed several years ago on a patient in our Outpatient ECG Lab. The patient was asymptomatic and the ECG was ordered as "Routine" by the patient's Primary Care Provider (PCP). I deliberately "froze" the tracing on the screen and captured this image because I wanted to show a transition on the ECG.
No clinical patient data available.
What does this tracing show? Choose the correct answer from the list below.
(1.) Patient with Wolff-Parkinson-White (W-P-W) syndrome and intermittent ventricular preexcitation. Sinus bradycardia with maximal preexciation on the first 3 beats. Lesser preexcitation on the 4th beat due to the Concertina effect. Normal conduction on the last 3 beats.
(2.) Junctional escape rhythm (i.e., junctional bradycardia) with left bundle-branch block (LBBB) aberrancy dissociated from a sinus bradycardia. Incomplete LBBB aberrancy on the 4th beat. Normal conduction on the last 3 beats.
(3.) Idioventricular escape rhythm on the first 3 beats, presumably originating from the right ventricle (RV) and dissociated from a sinus bradycardia. Ventricular fusion on the 4th beat. Normal conduction on the last 3 beats.
(4.) Ventricular demand pacing (rate about 40/min) from an Implantable Cardioverter-Defibrillator (ICD) and dissociated from a sinus bradycardia on the first 3 beats. Paced fusion on the 4th beat. Normal conduction on the last 3 beats.
(5.) None of the above.
HAVING TROUBLE ACCURATELY MEASURING THE DURATION OF INTERVALS, CALCULATING RATES, AND MARCHING OUT WAVEFORMS? NEED A PAIR OF CALIPERS TO ASSIST YOU? CLICK ON EITHER (OR BOTH) OF THIS LINKS TO START THE DOWNLOADING PROCESS.
FREE DOWNLOADS: ICONICO ECG SCREEN CALIPERS
(1.) http://fileforum.betanews.com/sendfile/970815244/1/1349998026.4c01f1f8f227433ec0a215146a507710ddf22096/Calipers.zip
(2.) http://www.abim.org/download/CaliperPearsonVue.exe
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
#3 is my choice for this one.
Thank you for these excellent cases.
zafer karabulut
Thank you!
. . . and thank you Zafer for your response! On behalf of myself and Dawn, you're certainly welcome! If you have any cases that you'd like to share, then you can forward them to Dawn at her contact information. Just make sure that you expunge all patient information. Please visit the Guru frequently since the two of us are always adding new material and cases on a weekly basis.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Thank you so much! Zafer
Thank you so much! Zafer
zafer karabulut
INTERPRETATION
The correct answer to this week's ECG Challenge is (3.)
INTERPRETATION:
(1.) Idioventricular rhythm (first 3 beats) presumably from the right ventricle (RV) dissociated from a . . .
(2.) . . . sinus bradycardia at a slightly faster rate (last 3 beats).
(3.) One ventricular fusion (F); 4th beat.
COMMENTS: Since both the sinus and ventricular escape rates are comparable, the A-V dissociation is termed "isorhythmic". The term isorhythmic is not rate-specific nor is it specific to only junctional mechanisms. It can also apply to ventricular mechanisms where the atria and ventricles are dissociated but are doing so at nearly identical rates. The first 3 beats with the wide QRS complexes illustrate the concepts of the so-called "Philadelphia Clue" and the "San Francisco Clue" popularized by Dr. Marriott. Respective to those clues, in lead V1, the QRS morphology favors LBBB since the nadir of the S-wave is reached in only 0.06s however the QRS morphology in lead V6 favors an ectopic ventricular origin since the peak of the R-wave is reached in about 0.10s. In light of the ventricular fusion on the 4th beat and the delayed peak in V6, this is undoubtedly a ventricular escape rhythm and not LBBB aberrancy. (1)
REFERENCE/SOURCE:
(1) http://heart.bmj.com/content/86/5/579.full#F8
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]