
Submitted by jer5150 on Sun, 12/09/2012 - 11:52
Patient's clinical data: 61-year-old black man.
What rhythm is this 12-lead ECG showing?
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
1. Normal sinus rhythm 2.
1. Normal sinus rhythm 2. Premature Junctional contractions 3. Complete RBBB. 4. Rightward axis.
Increased PR intervals after PJC's are due to concealed conduction.
zafer karabulut
couplets
Most of the SV ectopic impulses (I'm hedging my bet as to whether they're ectopic atrial or junctional) appear as couplets in a trigeminal pattern. i.e. sinus - sinus - sv couplet - sinus - sinus - sv couplet, etc. The fifth beat is the possible exception to this. However, even in this case the pattern may hold. The 5th beat is a sv ectopic impulse. If you consider the possibility that the notch at the end of the 5th QRS may be a non-conducted ectopic atrial P wave instead of a retrograde junctional P wave, then this cycle is also a sv couplet (the second of which is non-conducted) in the trigeminal pattern. This would also lead credence to these impulses being atrial, not junctional. Pieces fitting together. Interesting strip.
Walter A. Mueller, CCT, CRAT
Sinus Rhythm. The 5th beat a
Sinus Rhythm. The 5th beat a nonconducted APB. There seems to be a pattern of SV couplets in a
trigeminal pattern. RBBB pattern is also observed, with a Rightward Axis.
INTERPRETATION
INTERPRETATION:
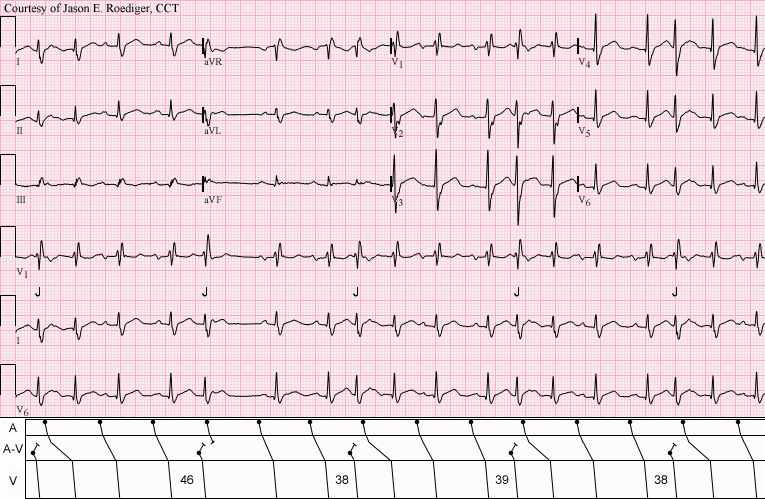
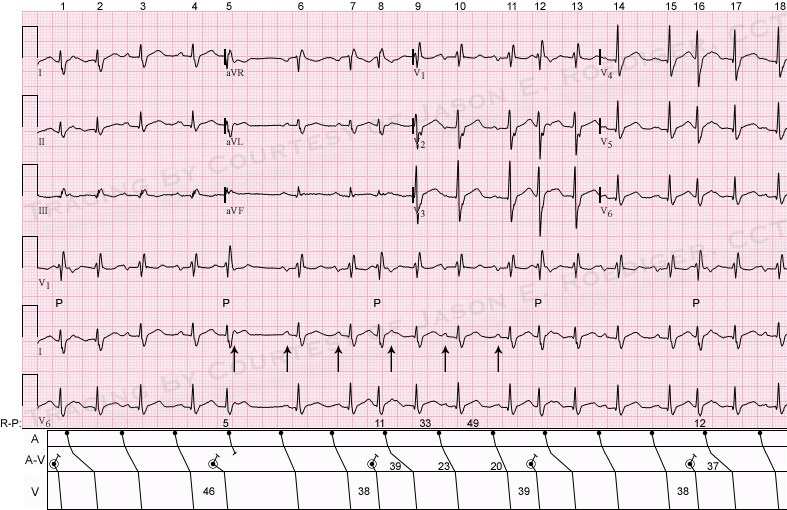
(1.) Sinus rhythm (rate about 84/min) interrupted by . . .
(2.) . . . five junctional premature beats (JPBs) with different “coupling” intervals and with . . .
(3.) . . . retrograde concealed conduction into the A-V node (see laddergram).
(4.) Right bundle-branch block (RBBB).
COMMENTS:
Four of the five JPBs are interpolated and none of them conduct retrogradely all the way back to the atria. Why is it that only the second junctional premature beat (J) is followed by a fully compensatory pause? The reason for this is simply because it has a measurably longer “coupling” interval of 0.46s whereas the remaining JPBs all have shorter “coupling” intervals of 0.38s to 0.39s. At a longer “coupling”, the associated R-P interval consequently shortens. As a result, the descending sinus impulse arrives at the A-V node when the tissue is still in its absolute refractory period. The interpolated JPBs all have "coupling" intervals that are sufficiently long enough that the sinus impulses arrive at the A-V node during its relative refractory period. Subsequently, this lengthens the ensuing P-R intervals to a much prolonged duration of about 0.36s. This is classic evidence of retrograde concealed conduction.
MY OWN INDEPENDENT OBSERVATION:
It has been my experience, that JPBs are more commonly seen when associated with bundle-branch blocks. In all cases, they never conduct retrogradely to the atria but rather they are either interpolated or they are followed by fully-compensatory pauses. I've seen them equally in the context of both right and left bundle-branch blocks. In my collection of ECGs, I have many examples of JPBs when the QRS is wide but virtually none when the QRS is normally narrow. While not seen here, parasystolic mechanisms are frequently associated with bundle-branch blocks as well.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Parasystole
It may also be worth mentioning that because the junctional discharges are regular and the coupling interval varies, this probably a junctional parasystole.
Dave R
Probably not
@Dave - You're exactly right that a parasystolic mechanism should always be considered when "coupling" intervals vary from beat to beat and are not fixed. Originally I had considered the possibility of junctional parasystole, however I don't think the interectopic intervals measure out convincingly enough to make that statement.
The first interectopic interval (i.e., J-to-J) measures 2.23s and the second interectopic interval measures 2.03s with a marked difference of 0.20s. If it had only varied by a mere 0.04s or so, then I would infer that possibility, but I think that the variability is too much here to postulate parasystole.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
probably not... but maybe?
Good point, Jason - I think I was a little sloppy in my measuring. However, desperate to salvage some pride, I wonder if there may still be a parasystolic mechanism but with slight variation in conduction time. In fact, given the normal rate of junctional discharge, I wonder if it may actually be a junctional parasystole with 2:1 exit block but I guess it's difficult to say. Keep up the good work!
Dave R
Another outstanding
Another outstanding observation that you bring up Dave! It's always refreshing to get other perspectives on ECGs. We don't exactly know the precise moment at which the A-V junction discharged since that specific information is concealed from direct view. In the laddergram's A-V teir, I've uniformly illustrated an identical anterograde (i.e., descending) conduction from the ectopic junctional focus (i.e., black dot). Conceivably, the second JPB, with the longest "coupling", could have discharged about 0.11s earlier than I've illustrated and then the black dots in the A-V teir would march out much more regularly. The interectopic intervals would then be in a more acceptable margin of irregularity. You may have motivated me to construct an "alternate" laddergram that will illustrate a junctional parasystolic mechanism. With regards to any potential 2:1 exit block, I'll have to research the discharge rate of junctional parasystole to determine if the manifest beats are occuring at typical rate. Stay tuned.
For any readers who are scratching their heads about the concept of "junctional parasystole", here is another laddergrammed image from the famed ECG Learning Center website: http://ecg.utah.edu/img/items/ecg_485.gif
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
autonomic modulation
Another thing that could contribute to the slight variability in inter-ectopic interval, if this is a parasystole, is modulation by the autonomic nervous system. A junctional discharge rate, like a sinus node discharge rate, is affected by varying autonomic tone. My money is on a junctional parasystole with 2:1 exit block and I'm looking forward to seeing what your research uncovers, Jason!
Dave R
Pieces fitting together
So much for my pieces fitting together. :)
Walter A. Mueller, CCT, CRAT