
Submitted by Dawn on Sat, 02/16/2013 - 18:52
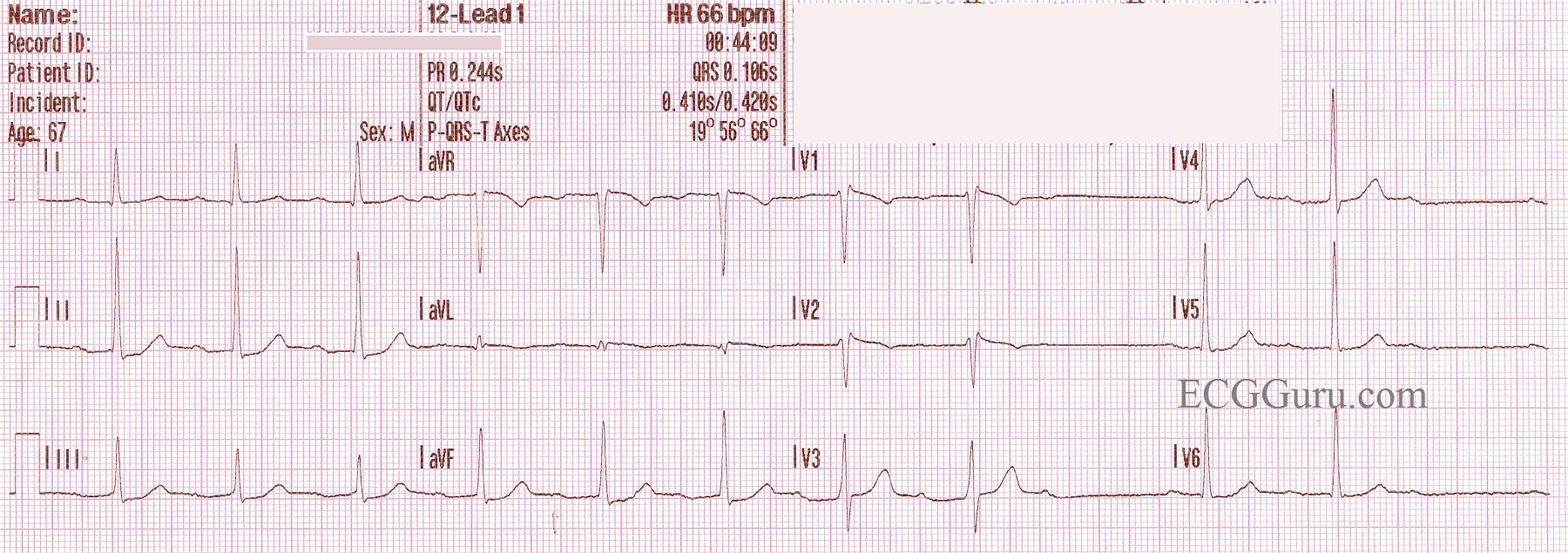
This 67 year old man is noted to have a slightly irregular pulse. At the beginning of this ECG, he appears to be in NSR with a first-degree AV block. Twice, P waves are non-conducted. Careful measurement of the P to P interval shows that it is regular, there are no PACs noted. The PR interval changes very subtly by lengthening just before the non-conducted P waves. A hint when non-conducted P waves are noted, first check for non-conducted PACs. If the sinus rhythm is regular, check the PR interval before the non-conducted beat, and the PR interval immediately after the non-conducted beat. You will see the PRI preceding the non-conducted P is longer than the PRI after the NCP.
Wenckebach conduction is caused by RP/PR reciprocity. In other words, the shorter the RP interval, the longer the PR interval. So, as the PRI lengthens, the QRS "moves" to the right, eventually causing the next regular sinus P wave to fall into the refractory period and fail to conduct. This results in a pause, or a long RP interval, which shortens the next PRI.
If you or your students would like to review AV Blocks, go to this LINK for Dr. Grauer's excellent, FREE, self-directed tutorial.
For a slightly more advanced discussion of RP/PR reciprocity, see Jason's Blog.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Subtle (Long-Cycle) AV Wenckebach
Dawn's Instructor tracing for this week provides a nice example of a long-cycle AV Wenckebach sequence. As per her description - this is a subtle form of Wenckebach - because there is minimal to no PR prolongation as one goes from beat-to-beat. It is only when one looks at the PR interval at the beginning of the sequence - and compares it with the PR interval at the end of sequence (just before the beat is dropped) that lengthening of the PR interval is seen.
As per Dawn - a KEY to diagnosing Wenckebach (and distinguishing Mobitz I from other entities such as blocked PACs and sinus pauses) - is that the P-P interval is constant. The other "footprint of Wenckebach" that I find especially helpful is that the pause containing the dropped beat is less than twice the shortest R-R interval (which it is here). Consideration of the phenomenon I call "birds of a feather" also helps. That is, we see a much-easier-to-recognize shorter Wenckebach cycle at the end of the tracing. This tells us this patient has a tendency toward Wenckebach - which has me strongly suspicious that any pauses I see elsewhere on the tracing are more likely than not to also represent a similar Wenckebach phenomenon.
Finally is the issue of "Why Wenckbach?" Mobitz I 2nd degree AV block is often seen with acute occlusion of the RCA (right coronary artery) - because the RCA most often supplies the AV node. While we do not see acute inferior infarction here - and while ST-T wave changes are admittedly subtle - I do believe there is slight-but-real ST elevation in lead aVL. Inferior ST segment straightening and ever-so-slight inferior ST depression may be a reciprocal change. Earlier-than-usual transition (the tall R wave in V3) may represent posterior involvement. So I'm suspicious that there may have been recent circumflex occlusion in a patient with a left dominant circulation resulting in postero-lateral infarction. Sequential tracings, troponins, additional rhythm strips and clinical course would be revealing as to whether the above suppositions are accurate. NICE tracing.
Ken Grauer, MD www.kg-ekgpress.com [email protected]