
Submitted by jer5150 on Sat, 03/16/2013 - 06:20
Patient's clinical data: Unknown aged white man.
What well-known eponym can technically be applied to this 12-lead ECG? HINT: It takes on a somewhat unusual form here.
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
JUN
Sinus rhy, with Jun exscape bradycardia approx. 50bpm, P waves seen in st seg. Inf st seg changes. Poss Inf wall MI
Had to ladder this one to be sure...
It was a bit tricky to confirm my suspicions and, as always, a ladder diagram proved invaluable. Cool tracing, especially since the "early" beats are actually the ones originating in the sinus node.
So, the underlying rhythm is sinus bradycardia at about 40 bpm.
This slow rate allows for a junctional rhythm to kick in at a rate of about 52 bpm. Usurpation by default.
This junctional pacemaker results in retrograde condution to the atria with varying 2:1 and 3:2 type I VA block, resetting the sinus node with each successful retrograde capture. It's also the source of the eponynm you're looking for: Wenkebach.
Vince D
http://www.medialapproach.com
Escape-Capture with Retrograde Wenckebach - GORGEOUS!
NICE interpretation by Vince!
GEORGEOUS example! - THANKS for posting - : )
Ken Grauer, MD www.kg-ekgpress.com [email protected]
more explainations please ?
can you please show with arrows the p wave ? thanks
1 2 3 viva l'Algérie vive MCO
@milerphile - This week's ECG
@milerphile - This week's ECG challenge was posted this past Saturday on March 16th. The interpretation and laddergram will be posted this coming Sunday on March 24th. I typically do this to allow an entire week's worth of time for members to respond.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Great case
Unfortunately I have read the answers already. Fascinating.
Looking forward to the laddergram.
Does this happen often? What to do with this clinically? Is it benign? Thank you!
INTERPRETATION
INTERPRETATION:1. Marked sinus bradycardia (rate indeterminate; probably in the 40s) with resulting . . .
2. . . . junctional escape rhythm (rate 51/min) and . . .
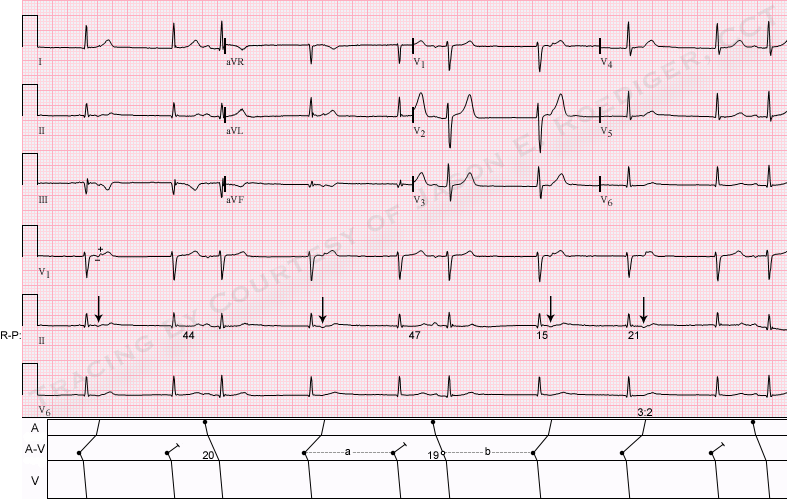
3. . . . 2:1 and 3:2 retrograde V-A Wenckebach period (see laddergram)
3. Probable old inferior infarction.
COMMENTS:
From the sound of his detailed description, I’m certain the Vince’s laddergram looks identical to the one I’ve constructed.
I would not call this “A-V dissociation by default” because A-V dissociation isn’t present here. The atria and the ventricles aren’t beating independently of each other. Whenever there is a sinus impulse, it successfully conducts to the ventricles with a normal P-R interval. As for the junctional escape beats, they either conduct backwards to the atria or they don’t but that would not qualify as A-V dissociation.
Beats 7, 8, and 9 represent a trio of junctional escape beats with 3:2 retrograde V-A conduction to the atria. Individually, beat 7 has an R-P’ interval of 0.15s. Beat 8 has an slightly but measurably longer R-P’ interval of 0.21s. Beat 9 does not conduct retrogradely and represents the equivalent of a “dropped” beat. The progressive delay is taking place at an anatomic level above the junctional pacemaker. Beats 1, 4, and 7 all display the same R-P’ interval. Beats 2, 5, and 9 are junctional escapes that are not associated with retrograde P’-waves.
Beats 1 and 2 as well as 4 and 5 represent pairs of junctional escape beats with 2:1 retrograde V-A conduction.
The early beats are not atrial premature beats (APBs) but rather (as Vince pointed out) they are actually conducted sinus beats.
The only primary finding is the sinus bradycardia and treatment should be geared towards treating that. The junctional escape rhythm is secondary.
As Vince also mentioned, the sinus node is unable to get a foothold or find a window of opportunity due to repetitive overdrive suppression by the consecutive discharges by the retrograde atrial activation.
As is often the case, all of the P-waves in lead V1 are diphasic. The retrograde P’-waves are (-/+) whereas the sinus P-waves are (+/-).
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]