
Submitted by Dawn on Wed, 03/27/2013 - 19:28
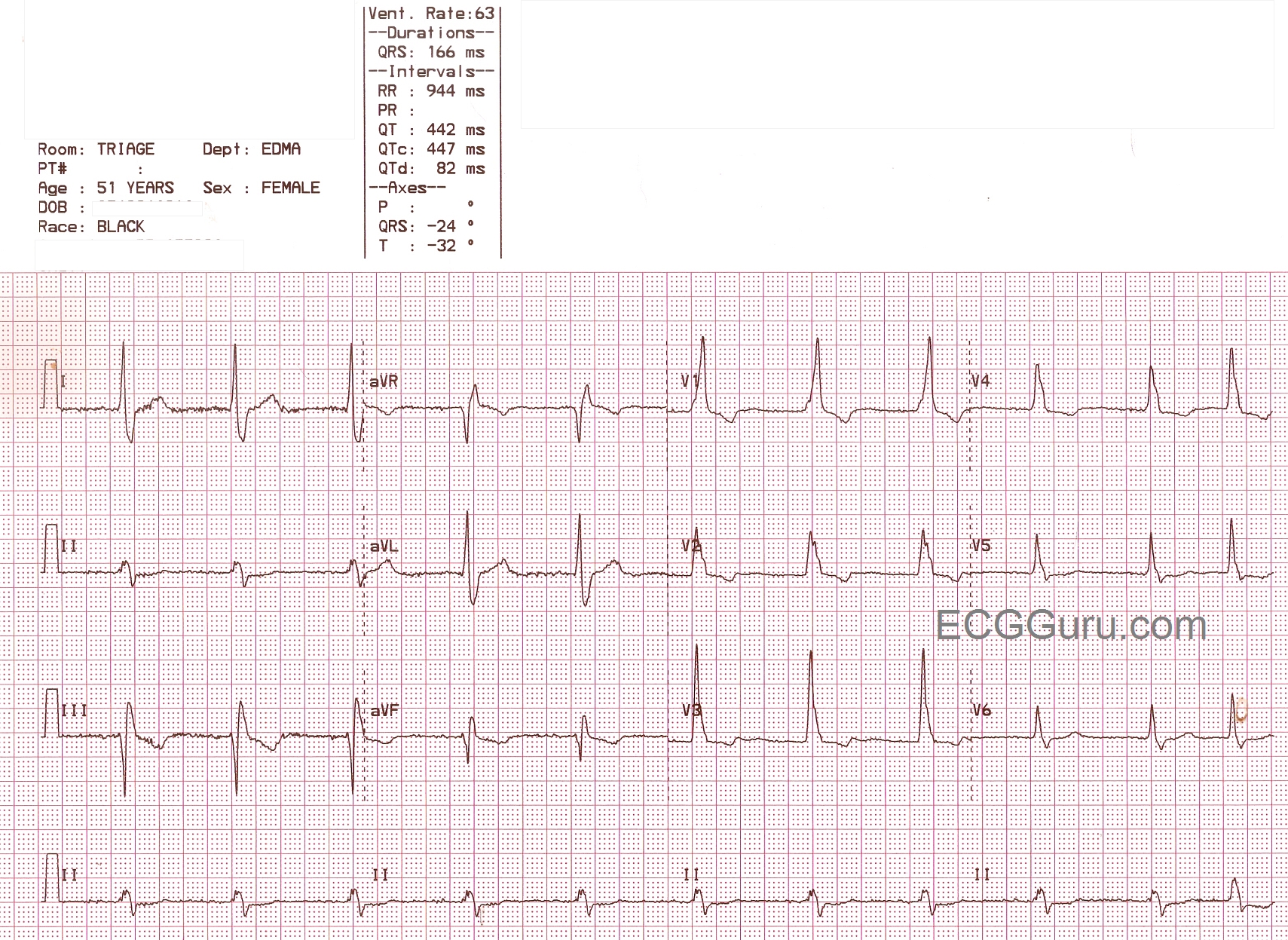
This is quite an interesting ECG, and the ECG Guru would love to hear what you think about it. What we do know is that it is a wide-complex bradycardia in a patient for whom we have no clinical data, except that she is a 51 year old female. The rhythm is probably junctional, as no P waves are seen and the rhythm is regular. The rate of 63 per minute would be consistent with that. Interestingly, no disassociated sinus P waves are seen. All slow wide-complex rhythms should be evaluated for idioventricular origin, or AIVR. The QRS in V1 shows an atypical right bundle branch block pattern. We usually look for rSR', or "bunny ears", but this ECG shows an upright R wave with a smaller, slurred r wave before it. What makes this look like RBBB is the prominent wide little S wave in V6 and in Lead I. We question the R wave progression, too. Do you think it is possible that the electrodes for V2 and V3 are switched? The axis is leftward, causing Lead II to be nearly biphasic - it represents a synthesis of what is seen in Leads I and III. This is enough left axis shift to diagnose a left anterior fascicular block (with RBBB = bifascicular block).
This is a great ECG, and we can't wait to hear from all you ECG Gurus out there. Maybe we will need to adjust our diagnosis after we hear from you.
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Tricky
As Dawn says, this is not a typical RBBB pattern and there are no definite P waves, whether normally conducted, dissociated or inverted due to retrograde atrial activation. As Dawn points out, the V2 and V3 electrodes appear to have been switched and in the lead that is labelled V3 I wonder if there is evidence of atrial fibrillation. Therefore, as an alternative to Dawn's suggestion, perhaps what we have here is AF with an accelerated idioventricular rhythm, possibly originating from the region of the left posterior fascicle.
Dave R
Great suggestion
Thanks, Dave. This pattern IS very suggestive of left posterior fascicle ventricular rhythm. The monomorphic V1 is a clue, as are the leftward axis. The precordial concordance makes me suspect VT, but not necessarily from the post fascicle. The lack of extreme left axis (aVR is neg) and the rarity of AIVR made me look for other explanations, but your suggestion makes a lot of sense. I wish we had an EP study! Thanks for your insight.
Dawn Altman, Admin
Third Degree AV Block, RBBB, LAFB with Junctional Escape
There is atrial fibrillation, yet a precisely regular ventricular rhythm so we obviously have a third degree AV block. I see no evidence of digoxin in the ST segments, so I doubt digtoxicity is playing a role here - though we do have block with a slightly accelerated junctional rhythm. I believe that there is a preexisting RBBB with LAFB (I am not concerned about the monophasic-appearing R in V1 since the wide, slurred S in Lead I says it all). If this were a ventricular escape rhythm or an AIVR, there would be more of an RBBB-like morphology, but not a true RBBB. The last beat comes early and - with its different morphology - is most likely a PVC. The rhythm is a junctional escape rhythm (though a tad bit fast) which would still be more common than an AIVR and certainly more common in the presence of a third degree AV block. I also agree that V2 and V3 have been switched.
Jerry W. Jones MD FACEP FAAEM
https://www.medicusofhouston.com
Twitter: @jwjmd
Thanks JWJ
Yes, I'm seeing the underlying atrial fib. So, CHB explains the regular escape rhythm. We have good arguments for both juntional escape with bifascicular block and for fascicular vent escape.
Still wish we had an EP study! Thanks for the interesting discussion.
Dawn Altman, Admin