
Submitted by jer5150 on Mon, 05/27/2013 - 11:40
Unfortunately, I have no available clinical data on this patient. Merely looking for an interpretation of the ECG in it's raw form.
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
3:2 type II AV block with PVC after the pause
Hope I dont look silly in front of the gurus
There are regular PP intervals, second degree type II AV block with 3:2 conduction. A PVC occurs after the first P wave after the pause causing it to be non conducted and AV dissociation to happen. QRS shows RBBB with typical strain pattern as well as probably sign of RVH.
Please enlighten
Ryan
Not a PVC
To quote the late-great Dr. Marriott, there's nothing "P" about that "VC". Those are indeed ventricular complexes (VC's) but they are most certainly not early. If not premature, what would they qualify as???
I disagree with the right axis deviation (RAD) being due to right ventricular hypertrophy (RVH). What else might account for the RAD in this specific situation???
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Jason thanks !!!
Jason thanks for your reminder it just strike my mind that this is a LPHB causing the RAD - so making this a bifascicular block
About the 'P'VC, that is why I said before hand I hope I dont look too silly in front of the gurus. Im not really sure what this if this is not a PVC. Would they qualify as just a ventricular escape rhythm ?
I hope Im not making myself sil(ier) with my comment
Thanks
Ryan
Think "passive" and "rescuing".
I now agree with your first sentence and your revised statement of LPHB instead of RVH. I should note that as of 2009, the AHA, ACC, and HRS no longer recommend use of the term “bifascicular” anymore. As an alternative, they recommend fully spelling out the specific part of the His-Purkinje system that is involved (e.g., RBBB+LAHB or RBBB+LPHB).
Both of these ventricular beats are manifesting at the end of cycles that are longer than the basic sinus cycles and only occur after "dropped" beats. In other words, they are terminating pauses. Since they are occurring in isolation (i.e., singly), they would only be called ventricular escape beats and not a ventricular escape rhythm which is when ventricular escapes happen in succession (i.e., consecutively).
If you already have a copy of this book in your personal library, I would recommend reviewing this case (fig. 10.14) on pages 132 and 133 of Dr. Marriott's 8th edition of Practical Electrocardiography. This is where a obtained Dr. Marriott’s previous quote.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Thanks
Thanks for the pesrl
Unfortunately my order from eBay has been lost but I ave been trying to get a copy off this book right now..
Ryan
Mobitz II - Successive Dropped P waves / Vent. Escape
NICE tracing and well described by Jason! I'll just add a few points about this interesting tracing.
GREAT teaching tracing!
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Lead V6
Ken,
If you wanted to evaluate the QRS morphology of the conducted sinus beats in lead V6, the 3rd monitoring lead at the very bottom of the ECG is a long version of that particular lead. Before I obtain a screen capture of these digital ECGs, the bottom lead always default to lead V5. I almost always manually change it to lead V6.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Mobitz II 2nd Degree AV block description???
Hi guys.
I am new to the site and am currently training as a cardiac physiologist in the UK. Just warning you that I will no doubt be bombarding you all with ECG Q's in the future! So be warned!
May I start by complementing the quality of the recording above and also the interesting nature of ECG. Thankyou for sharing!
The attempted ECG interpretation that follows is that which I initially formulated prior to reading the comments, and a question does arise....
Underlying sinus rhythm with 1st degree AV block, RBBB, and LPHB. Mobitz II 2nd degree AV block (4:2 conduction) with a ventricular escape beat noted following every second non-conducted sinus beat.
The general terminology I have used is possibly different than the descriptions above and maybe due to regional variability, but I think we are basically in agreement on the fundamentals.
I do recognise that I may be going wrong on the description of Mobitz II 2nd degree AV block. Please advise....
The question that I propose is: Can the Mobitz II 2nd degree AV block in the ECG above be described as 4:2 conduction?
My reason for this is that there are 2 x non-conducted sinus beats following 2 x conducted sinus beats (4 x sinus beats with 2 x successive conducted/non-conducted sinus beats)....4:2 conduction?
Any advice would be much appreciated.
WayneB
Welcome
Greetings Wayne from "across the pond"! I'm going to eventually address your questions when I get a chance to and I'll be providing a full interpretation in the near future. Again, welcome to the ECG Guru!
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
I would also say that this is
I would also say that this is Mobitz type II, 2nd degree AV block with a Ventricular escape beat with every pause.
Dr Stasinos Theodorou
MB ChB, MRCP(UK)Interventional Cardiologist
www.cardiolimassol.com
2 consecutively blocked P's?
In regard to the 2 consecutively blocked P waves, I assume the second is the one immediately preceding the ventricular escape beat in each case? If I am correct in that, can that P wave definitely be linked to the pathological block? Isn't it possible and even likely that it is interfered with not by the pathological block but rather by the dissociated ventricular escape beat? I would still agree with Mobitz II vs. Mobitz I because I do not see any PR prolongation, but I am confused on this point about the consecutively blocked P waves. Thanks for your help.
Walter A. Mueller, CCT, CRAT
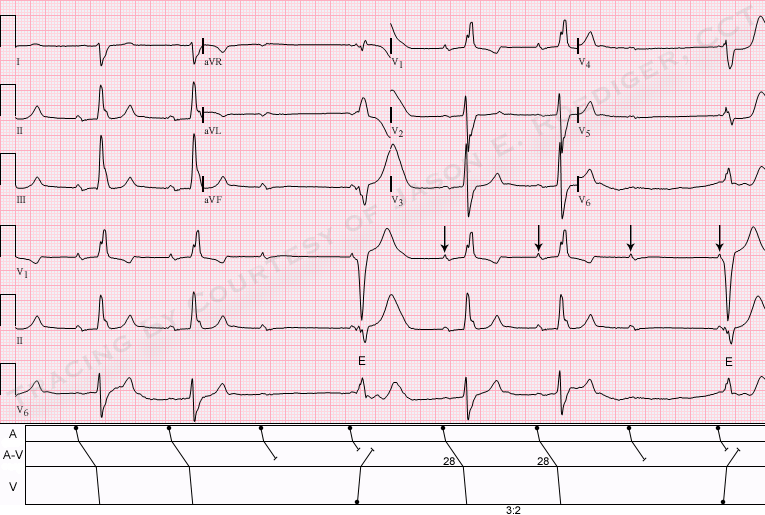
INTERPRETATION
INTERPRETATION:
1. Sinus bradycardia (rate about 48/min) with . . .
2. . . . Type II A-V block.
3. Right bundle-branch block plus left posterior hemiblock (RBBB+LPHB).
4. Two ventricular escape beats presumably originating from the right ventricle; (see laddergram.)
COMMENTS:
I would not define this as high-grade (or advanced) A-V block. I agree with Walter Mueller that the nonconduction of the 4th and 8th sinus impulses is not due to pathological A-V block. Dr. Marriott's criteria for diagnosing high-grade A-V block is when, at reasonable atrial rates, two or more consecutive atrial impulses fail to be conducted because of the block itself - and not because of interference by an escaping subsidiary pacemaker. The 4th and 8th sinus impulses are not given a fair chance to conduct because the relationship between the sinus impulse and the ventricular escape is foreshortened due to dissociation between the atria and the ventricles. We are already able to establish that the P-R interval on the conducted beats is somewhat prolonged. We have no way of knowing for certain, but the 4th and 8th sinus impulses probably would have conducted had the ventricular escape beats not manifest.
With regards to WayneB's question, I would not describe the ratio as 4:2 but rather 3:2. I would not factor the dissociated sinus impulse into the ratio for the reason I've listed above. The 4th and 5th QRS complexes together with the 5th, 6th, and 7th sinus P-waves comprise a ratio of 3:2.
The prolonged P-R interval on the conducted beats could be due to either delay within the A-V node or it could be due to infranodal block in either the His bundle or the left anterior fascicle (LAF). The "dropped" beat could be due to block at the anatomic level of the His bundle but are probably due to block in the left anterior fascicle.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]