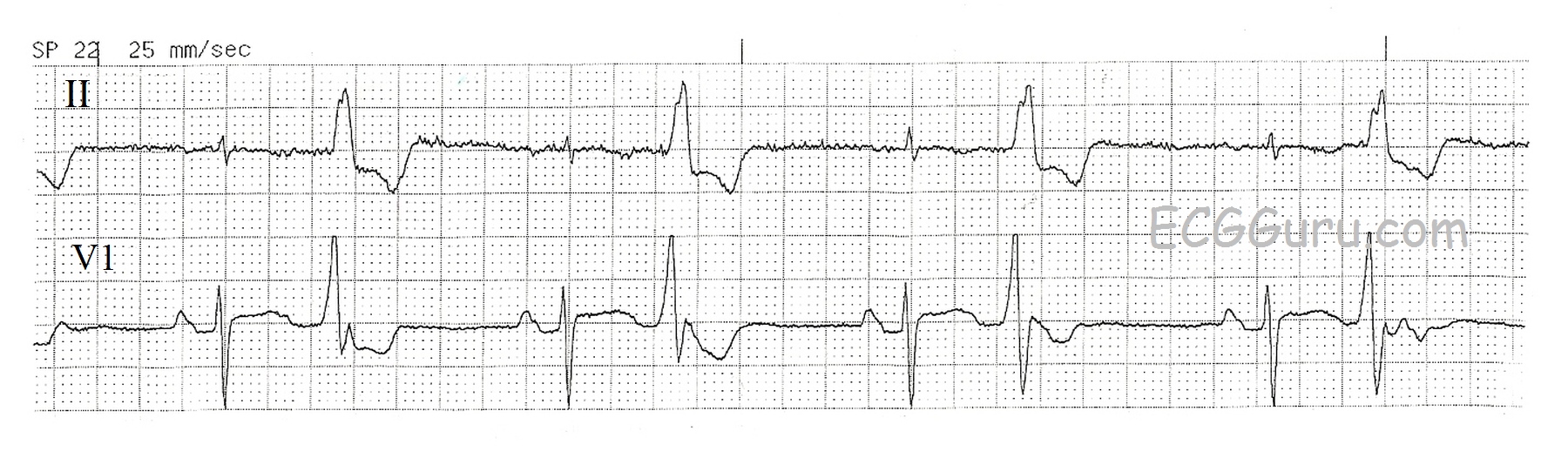
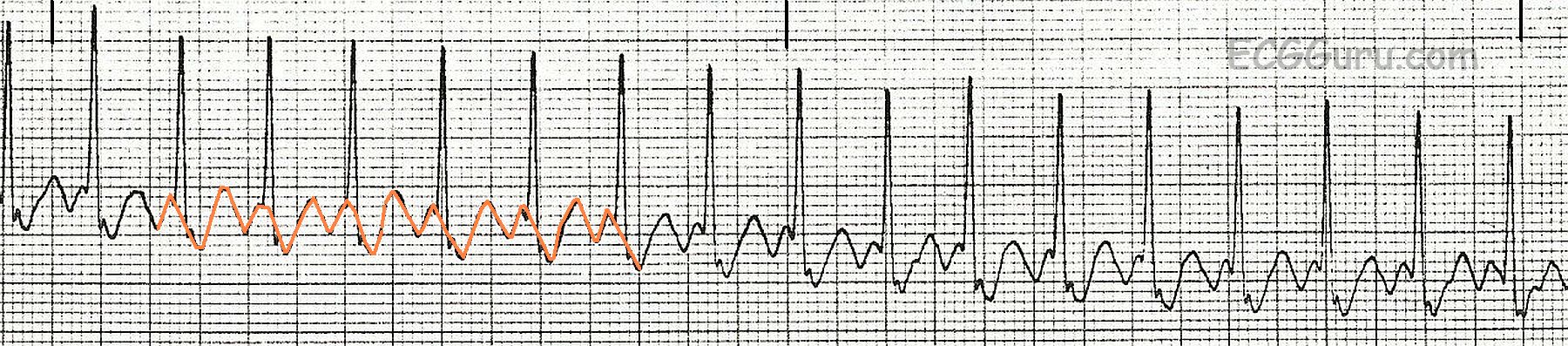
This two-lead rhythm strip clearly shows the transition from normal sinus rhythm to a paroxysmal supraventricular rhythm. In this case, the arrhythmia is AV nodal reentrant tachycardia, AVNRT. The rate of the first rhythm, NSR, is around 75 per minute. The fourth beat on the strip is a PAC which initiates the paroxysm of tachycardia lasting 12 beats. The arrhythmia terminates spontaneously at that point. The tachycardia rate is about 150/min.
The topic of supraventricular tachycardias can be a very complex one to teach. For an excellent example of a concise lesson geared toward Primary Practice physicians, go to Dr. Grauer's VIDEO - Part III of his Arrhythmia series.
To cover the important points for the beginner-level student:
* It can be difficult to determine a rhythm is SVT if the rhythm is near 150 bpm and you DON'T see the beginning or end of the arrhythmia. If the onset (or offset) is sudden, then this is not a sinus rhythm. The sinus node speeds and slows more gradually - it doesn't change rates in one heartbeat. This strip has an excellent view of BOTH the onset and the offset.
* The faster the rate, the more likely we are looking at a PSVT rather than sinus rhythm. If a sinus tachycardia exists, we can almost ALWAYS see the reason for it in the patient's clinical situation. We may see fever, dehydration, bleeding, fear, pain, exercise. Therefore, a patient at rest with a rate of 150 would be suspect for PSVT. A patient on a treadmill for 5 minutes would be considered to have a sinus rhythm.
* Any patient with a rate around 150 per minute should be evaluated for ATRIAL FLUTTER with 2:1 conduction. Atrial flutter often conducts at that ratio, because a rate of 150 is fairly easy for the AV node to conduct, whereas the instrinsic rate of atrial flutter (250-350) is not. A 12-lead ECG makes it easier to search for tell-tale flutter waves.