A good example of ventricular fibrillation. The patient is pulseless, CPR has been performed, and the ED staff is about to defibrillate. Characteristics of V Fib are: a chaotic, wavy baseline without clear P waves, QRS complexes, or T waves. Baseline artifact (baseline going up and down) can be seen with CPR and other movement of the electrodes on the patient's body as resuscitation efforts are underway. The patient will ALWAYS be unconscious and pulseless in V Fib. If this rhythm is seen in a patient who is awake or has pulses, it is ARTIFACT - check your electrodes!
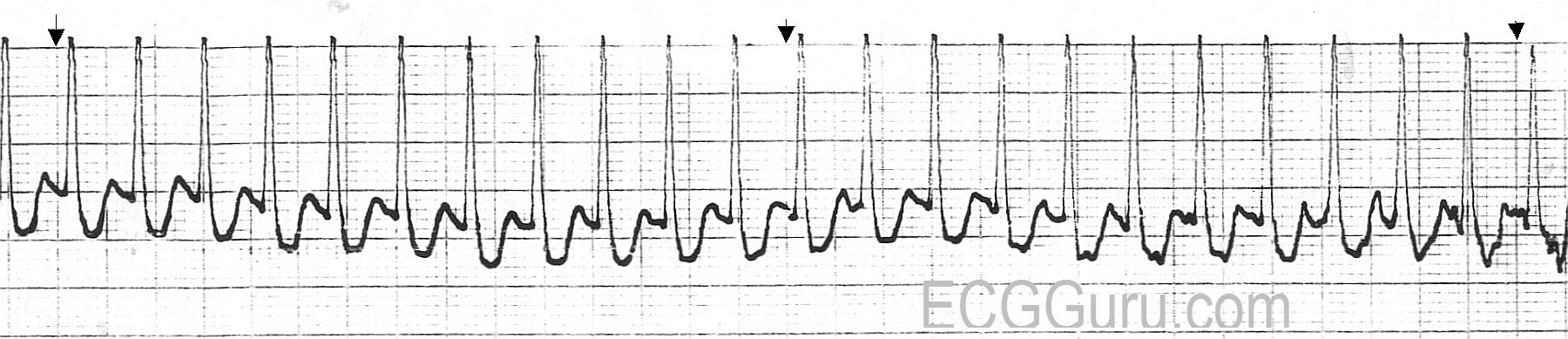
Today, you get THREE strips for your basic classes! The first shows a PSVT - paroxysmal supraventricular tachycardia at a rate of about 220/minute. The QRS complexes are narrow, and the rhythm is regular. In the second strip, we see the moment of conversion after a dose of 6 mg. of adenosine was administered by rapid I.V. infusion. The re-entry cycle is broken, and the patient experiences many PVCs, including groups of two, three, and even four in a row. Soon, however, the rhythm settles into sinus rhythm with PACs, and later, just sinus rhythm (not shown). For your more advanced students, the second strip shows the PVCs interacting with the underlying sinus rhythm. There are several fusion beats with varying degrees of fusion, and one can sometimes see a sinus P wave just before a PVC. None of this is clinically significant in this patient, because the ventricular ectopy was a side effect of the treatment, and was self-limited. It is a great strip for teaching, though!
This rhythm strip illustrates a junctional escape rhythm. The sinus rhythm has slowed or stopped, and the junctional tissue has taken over as the pacemaker of the heart. The "junction" is loosely defined as the area between the AV node and the Bundle of His. The intrinsic rate of the pacemaking tissue in this area is 40 - 60 beats per minute. This slow rate is usually overridden by the sinus node, and the junction is not allowed to express itself as a pacemaker. Should the sinus node fail or fall below the junctional rate, the junction "escapes" and takes control of the heart. The QRS complex in junctional rhythm will normally be narrow, because the impulse follows the bundle branches down through the ventricles in a normal fashion, resulting in quick and normal ventricular depolarization. If the QRS complex is wide in a junctional rhythm, there is another, separate cause, such as bundle branch block.
If the junctional impulse is able to penetrate the AV node and depolarlize the atria, the P wave will be deflected downward in Leads II, III, and aVF, as the impulse is travelling in a retrograde direction (backward). The P wave could end up slightly before the QRS, during the QRS, or after the QRS. In this strip, the P waves are seen after the QRS complexes.
This is a good teaching strip for showing your students how to "see" the atrial activity separately from the ventricular activity. The P waves, also called flutter waves, march out regularly at a rate of around 300/minute, which is typical of atrial flutter. The conduction ratio is variable, and the intervals between the conducted P waves and the QRS complexes vary, as well, reflecting changing refractoriness of the AV node. It is easy with this strip to "march out" the flutter waves, through the QRS complexes, and to show your students how the flutter waves are either visible, or "hiding" behind a QRS complex. We have featured several atrial flutter examples on the ECG Guru recently. Remember, you can also obtain rhythm strips for your basic students by cropping out the rhythm strips often found at the bottom of 12-lead ECGs.
An example of ventricular tachycardia in Lead II. This patient's rate is about 190/min. V Tach will have the following criteria: Rate greater than 100/min, QRS duration greater than .12 sec. (120 ms), and no P wave associated with the QRS.
It can be difficult to distinguish V Tach from other wide-complex tachycardias without a 12-lead ECG, but all wide-complex tachycardias should be treated as V Tach until proven otherwise, as V Tach is a potentially lethal dysrhythmia. V Tach can cause a severe reduction in cardiac output which can lead to V Fib and death.
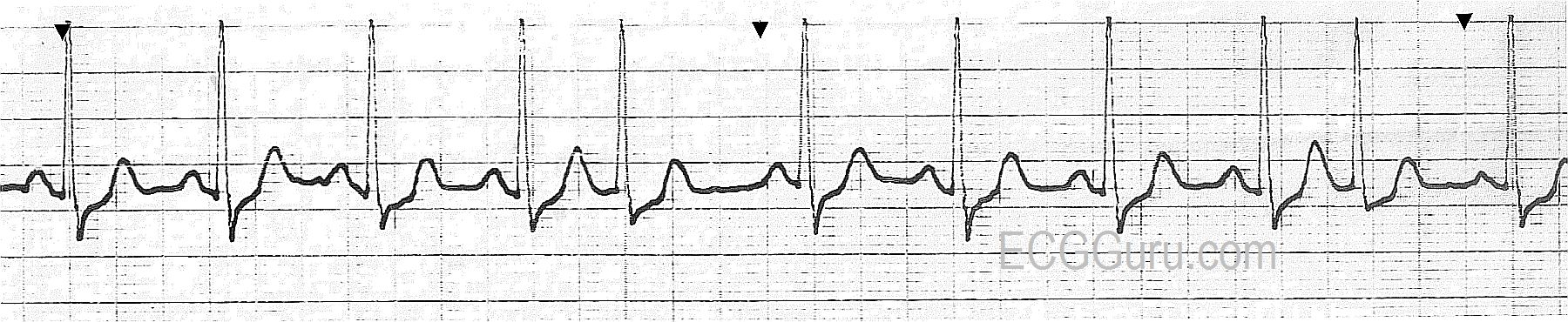
This Lead II rhythm strip was taken from a 12-Lead ECG performed on a 66-year-old man who was having an acute inferior wall M.I. The rhythm is normal sinus rhythm at 65 bpm. The QRS complex is slightly wide at 112 ms (.11 seconds). The patient did not have a bundle branch block pattern on his 12-lead ECG. The PR interval is .17 seconds, and the P waves are widened and have a "double peak". This can be a sign of left-sided heart failure, and is called P Mitrale. Your students should be advised not to try to diagnose acute M.I. from a monitor strip, as ST segments can be inaccurate on some types of monitors. However, any derangement of the ST segment on a monitor strip calls for an immediate 12-Lead ECG for confirmation.
This is a Lead II rhythm strip from a patient with a biventricular pacemaker. The second and sixth beats are PVCs. In this lead, the pacemaker spikes are very difficult to see, but they are present. The pacemaker is operating in a "demand" mode for pacing the atria. Some of the P waves appear to be the patient's own, and some appear to be caused by the pacing stimulus. For example, the first beat appears to have no pacer spike before the P wave, and the second beat does have one (albeit tiny). The morphology of the P waves appears to change, also.
This pacemaker has been programmed to cause a QRS complex after every P, whether the P wave was made by the patient or by the pacemaker. The patient originally had a left bundle branch block, making his QRS complexes very wide, and lowering his cardiac output. The biventricular pacemaker paces both ventricles, synchronizing their depolarization and narrowing the QRS. This improves cardiac output. The physician has programmed this pacemaker to pace the ventricles after every P wave, whether native or paced. The paced QRS happens slightly before the native (wide) QRS would have, giving the patient the benefit of narrow QRS complexes. Biventricular pacemakers have been shown to improve cardiac output in patients with wide complexes.
Up until now, we have posted basic rhythm strips in this area of the ECG Guru for those of you who are teachers of beginning students. Today, we offer a "normal" 12-Lead ECG for those desiring to introduce students to the 12-Lead format. It is always best to become familiar with normal before venturing into the realm of "abnormal". Encourage your students to find what they know to be normal, then add to their knowledge. Examples of findings which are within normal limits are: rate, rhythm, P wave morphology, QRS morphology, intervals, axis, R wave progression, ST segments, and T wave direction.
While advanced practitioners can almost always find something that is not "normal", we must remember that that can be said about almost any human body. This ECG was taken from a healthy volunteer with no medical complaints.
This rhythm strip shows a good example of complete (third-degree) AV block with ventricular escape rhythm. It will be easy for your basic students to "march out" the P waves. They are regular at a rate of about 88/min., and they are either visible, or are "hiding" in the QRS complex. The ventricular rhythm is wide and very slow, and completely dissociated from the sinus rhythm.
For your more advanced students, you may want to discuss the likely origin or "level" of the block. Blocks above the Bundle of His can have JUNCTIONAL escape rhythms, while blocks that occur below the Bundle of His generally have ventricular escape rhythms. Ask your students which type of CHB they would prefer to have: suprahisian or subhisian - and why?
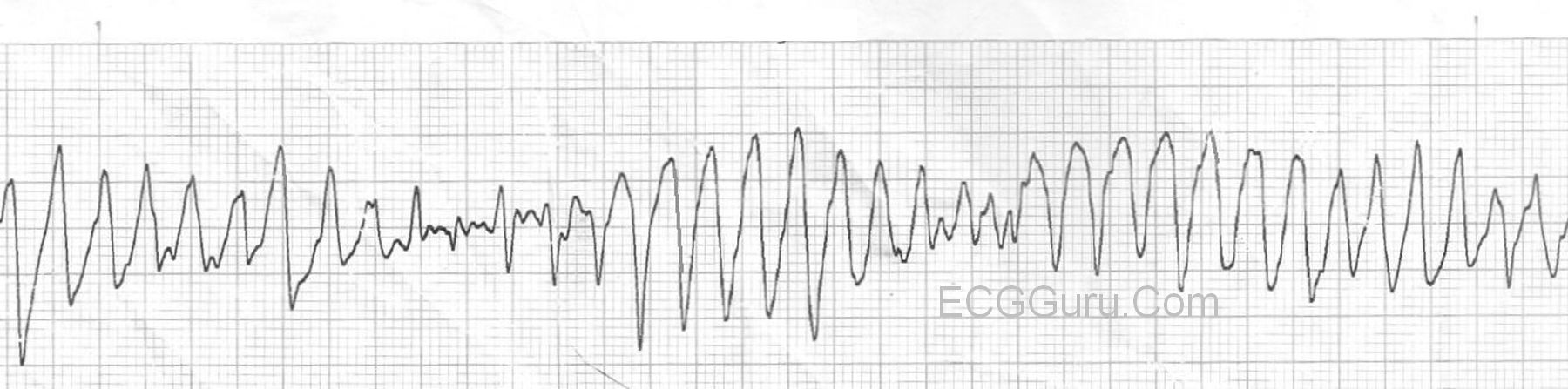
Torsades de pointes, or polymorphic ventricular tachycardia, is a ventricular tachycardia precipitated by and associated with long QT Syndrome. Long QT Syndrome can be congenital or acquired. Torsades is life-threatening, and can be made worse by many drugs, including some of the drugs used to treat VT. The rate is usually 150 - 250 / min. and the appearance is of a wide-complex tachycardia with QRS morphology changes. In some leads, it will appear as if it is "twisting" around the isoelectric line, giving it the French name, Torsades de pointes, a ballet term meaning twisting of the points. For a thorough discussion of Torsades, check this LINK.