
Submitted by Dawn on Wed, 05/06/2026 - 16:50
The Patient: This ECG was obtained from a 29-year-old man who was found by his wife, prone on the floor. He was unresponsive. When paramedics arrived, they found him to be in V fib. He was shocked at 360 J twice, with no conversion. The third shock was delivered using the dual sequential method, delivering 720 J. That shock resulted in conversion to the rhythm you see here. We don’t have information on any previous medical history, or on the outcome of the patient after he was transported to the hospital. During transport, he received Esmolol 40 mg IVP and Amiodarone 150 mg in 50 ml, administered over ten minutes.
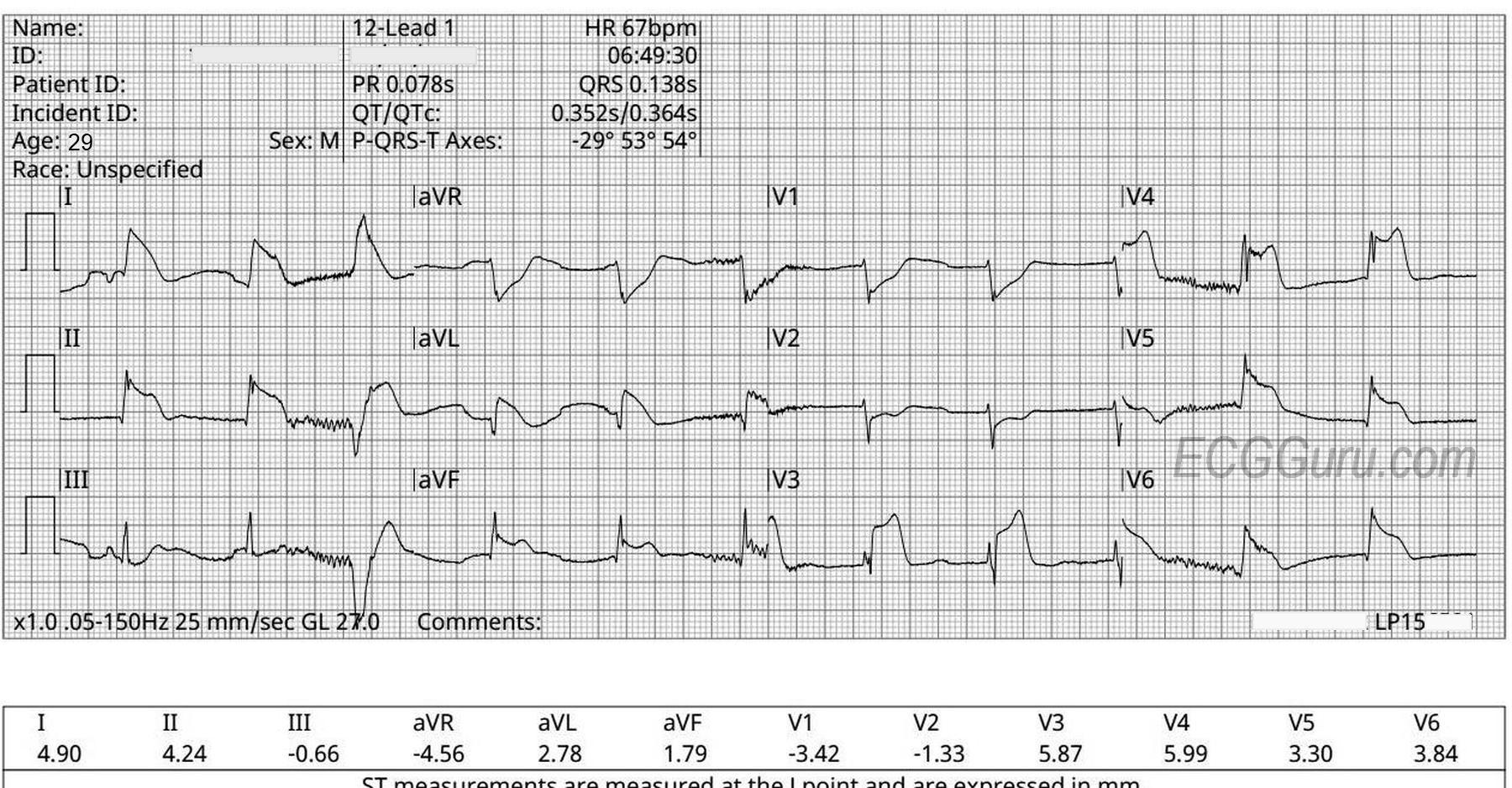
The ECG: The rhythm is regular, except for one slightly-early beat, third beat in. The only P wave seen is in the first beat, and the axis of that P wave is very rightward (negative in Lead I). This could be an artifact, or represent an atrial ectopic beat. There are no obvious signs of lead misplacement. Without P waves, this regular rhythm would have to be called accelerated junctional rhythm. Since this man was just shocked three times, at high doses, I would want to let the rhythm “settle” a bit before deciding what to name it. For now, it is fast enough to produce pulses, and a workable BP, and not so fast as to stress the heart. I would be satisfied with that for the time being.
The ECG machine measures the QRS duration at .183 seconds. This is the width of that one stray ventricular beat – technically a PVC, but late enough to have some escape characteristics. The rest of the QRS complexes on the page are quite narrow: about .07 seconds, or 70 ms. See Leads III, V1 and V2. Remember, the channels on this ECG are run simultaneously. The beats shown in a vertical stack are the same beat, and will have the same intervals as the other beats in that vertical line.
So, what made the QRS complexes look wide and fool the machine?
There is significant ST elevation in the following leads: I, II, aVL, aVF, V3, V4, V5, and V6. The ECG machine agrees. There is also reciprocal ST depression in aVR, V1, and V2. And possibly a little in Lead III, though it is more of a sagging shape than J point depression. This is the pattern of a large posterior-lateral occlusive myocardial infarction (OMI). We know that this patient had a period of pulselessness due to V fib. Signs of ischemia, even Type II OMI (not due to a blood clot), are definitely a possibility after such trauma to the heart. There is also the possibility that the patient had a massive OMI, probably due to occlusion of the circumflex artery or it’s branches, and that OMI caused the V fib. The machine has mistaken the dramatic ST elevation for wide QRS complexes. This OMI pattern should be considered to be an acute OMI until proven otherwise. Since we have no follow up on this patient, we do not know for sure. I will update this comment if I receive more information.
UPDATE: This patient went to the cardiac cath lab, where no coronary artery disease was found. He recovered without neurological sequelae, and was discharged home. This very happy outcome has left us wondering if he had: 1) Ischemic changes from pulseless period, 2) Myocardial infarction with no obstructive coronary artery disease (MINOCA), or 3) pulse-tap artifact (PTA). We will never know for sure. Some links for further study of this topic: https://drsmithsecgblog.com/repost-63-minutes-of-ventricular/
https://ecg-interpretation.blogspot.com/2021/03/ecg-blog-201-ecg-mp-18-s...
https://ecg-interpretation.blogspot.com/2024/02/ecg-blog-415-cath-showed...
Our thanks to Ashley Terrana for donating this teaching case.
Related Terms:
Rate this content:
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Why Cardiac Arrest in a 29-year old?
Interesting case of a 29-year old who was found by his wife to be unresponsive — in VFib on arrival of the paramedic team at the patient’s house. 3 shocks were required until restoration of a supraventricular rhythm.
I agree completely with Dawn’s interpretation. Because of the clinical circumstances of this patient’s cardiac arrest, as well as the dramatic findings on this post-resuscitation tracing — I thought it would be insightful to review the excellent points raised by Dawn.
Marked ST elevation in leads such as I,II,aVL; and V3-thru-V6 renders assessment of QRST morphology difficult until we appreciate that the “shark-fin” morphology in the above leads simulates QRS widening because of the huge amount of ST elevation. But (as per Dawn) — simultaneously-recorded leads III, aVF, and V2 tell us that the QRS is really narrow.
So we have a 29-year old man who was found unresponsive and in VFib — with dramatic ST elevation in multiple leads on restoration of sinus rhythm. So, while I completely agree with Dawn’s caution and her wanting to wait a few minutes while allowing the rhythm to “settle” down before jumping to an assessment — I would definitely be thinking about the need for prompt cath to define the anatomy. Practically speaking — by the time it would take to activate the cath lab — you will KNOW if the ECG will truly “settle” That said, given the young age of what seems to have been a previously healthy young adult — and what looks like an extensive acute infarction on this initial post-resuscitation ECG — it’s hard to imagine that prompt cath won’t be clearly indicated.
I agree with Dawn that the only potential indication of atrial activity is probably the result of artifact (ie, the negative deflection before the 1st beat in lead I — and the positive deflection before beat #3 with resultant flat line in lead II is simply not consistent with an expected arial morphology).
The 3rd beat is a late-cycle PVC — which is remarkable for the primary ST elevation in lead II — by itself is diagnostic of acute infarction.
Finally — I agree with Dawn that I’d look first for an acute dominant LCx artery occlusion as the cause for this patient’s event. Small Q waves are already forming in multiple leads. The ST depression in leads V1,V2 argues again a proximal LAD occlusion. While I could not eliminate the possibility of a more distal LAD occlusion — I thought acute occlusion of a dominant LCx a far more logical “culprit” artery. But this is all academic. Because this patient is going to need prompt cath.
Ken Grauer, MD www.kg-ekgpress.com [email protected]