The Patient:This ECG was obtained from a 29-year-old man who was found by his wife, prone on the floor. He was unresponsive. When paramedics arrived, they found him to be in V fib.He was shocked at 360 J twice, with no conversion.The third shock was delivered using the dual sequential method, delivering 720 J.That shock resulted in conversion to the rhythm you see here.We don’t have information on any previous medical history, or on the outcome of the patient after he was transported to the hospital.During transport, he received Esmolol 40 mg IVP and Amiodarone 150 mg in 50 ml, administered over ten minutes.
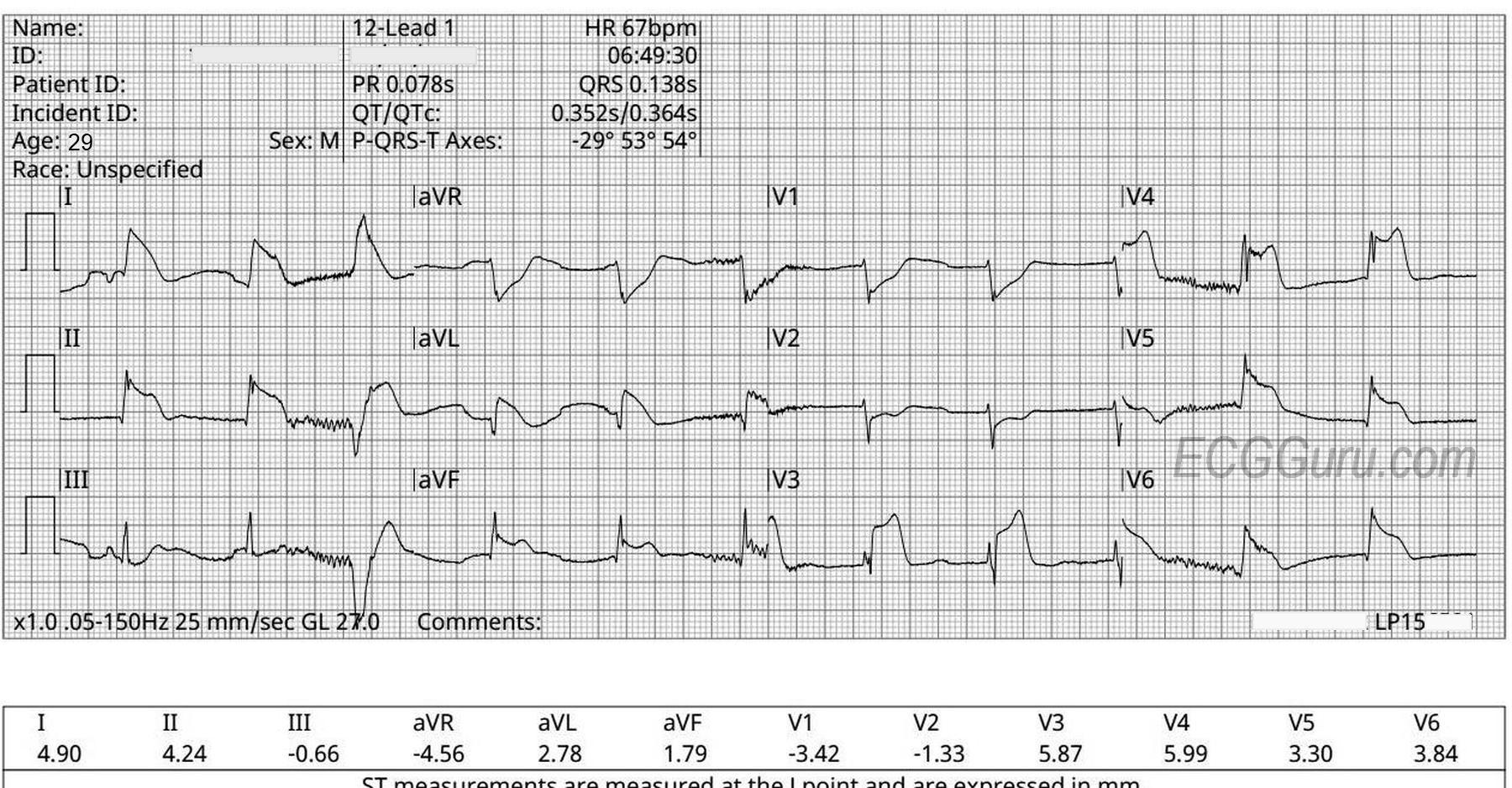
The ECG: The rhythm is regular, except for one slightly-early beat, third beat in. The only P wave seen is in the first beat, and the axis of that P wave is very rightward (negative in Lead I). This could be an artifact, or represent an atrial ectopic beat. There are no obvious signs of lead misplacement. Without P waves, this regular rhythm would have to be called accelerated junctional rhythm. Since this man was just shocked three times, at high doses, I would want to let the rhythm “settle” a bit before deciding what to name it. For now, it is fast enough to produce pulses, and a workable BP, and not so fast as to stress the heart. I would be satisfied with that for the time being.
This strip shows a junctional rhythm at a rate of 110 beats per minute. The QRS complexes are slightly wide at .10 seconds (100 ms), and they are within the parameters for supraventricular rhythm. The term, "junctional tachycardia" could be used, also, but this is not likely a "reentrant" junctional tachycardia, which would be fast, regular, and have a sudden onset. That type of junctional tachycardia is a PSVT. In this strip, we can see the underlying sinus rhythm in P waves that appear to pop up randomly. However, if you march out the P waves, you will find that they are regular, at a rate of about 90 per minute. The junctional rhythm has overrun the sinus rhythm. Most of the P waves cannot conduct due to where they have landed - in the refractory period of the QRS. The exception might be the P wave after the fifth QRS. The sixth QRS might be conducted from that P wave.
When accelerated junctional rhythm is encountered, you should suspect DIGITALIS TOXICITY - the classic dysrhythmia associated with digitalis toxicity is accelerated junctional rhythm. Other causes in adults could be beta-agonist drugs such as adrenalin, cardiac infection, ischemia, or surgery.