The Patient: 67-year-old man complaining of chest pain radiating to his jaw, 10/10. He is short of breath and diaphoretic. We do not know his BP, just that it was low. The patient states “no past medical history – never hospitalized”. He thought himself to be very healthy. He was given aspirin 325 mg and transported to a full-service cardiac hospital as a “cardiac alert”.
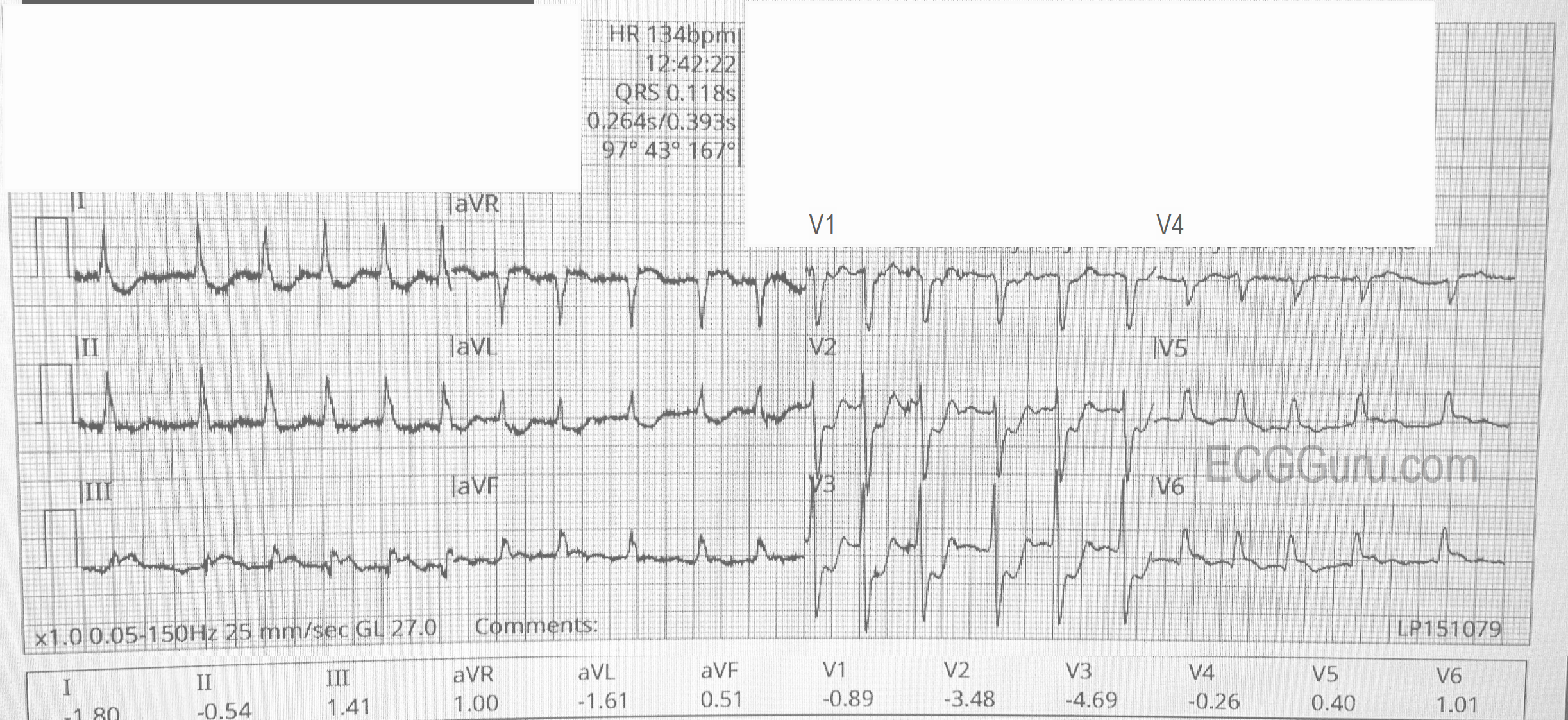
The ECG (from EMS):
The rhythm is atrial fibrillation with a rapid ventricular response (about 134/min.). The QRS width is .118 seconds (118 ms). The frontal plane axis is slightly to the left, but WNL. The R wave progression mostly normal, but V4 is incongruous. V2 and V3 have a tall R wave, possibly representing a pathological Q on the posterior side. There are ST CHANGES in every lead. ST elevation is noted in III, aVF, aVR, V5 and V6, representing ischemia in the inferior wall. There is ST depression in all other leads, indicating widespread subendocardial ischemia and/or acute reciprocal depression. Interesting that Lead II would normally be elevated when III and aVF are, but aVR is elevated, causing reciprocal ST depression in Lead II. So, Lead II looks almost normal.
The pattern of ST elevation in aVR with widespread ST depression can indicate:
1) Proximal occlusion of LAD or significant stenosis of Left Main artery.