
Submitted by jer5150 on Sat, 10/13/2012 - 17:20
A member’s recent comment inspired me to post this ECG. I’ve chosen this topic because there is much confusion and misunderstanding about it.
Beginning with this ECG of the Week, I’m going to start routinely presenting these as multiple choices in order to try and encourage more active participation from ECG Guru members. I copied the idea from one of Dr. Wang’s ECGs that was posted on Medscape 8 years ago.
This was one of five consecutive ECGs that I performed on a patient a month or two ago.
Patient’s clinical data: 68-year-old white man with unremarkable cardiac history. After his primary care provider (PCP) detected a slow and irregular pulse on this patient, she sent him over to me, in the Outpatient EKG Lab, to perform a “routine” 12-lead ECG.
Pick the answer that you feel best describes what is seen in the ECG above:
(1.) Starts out as Type II, converts to Type I, and then reverts back to type II AV block
(2.) Type I AV block all throughout
(3.) Type II AV block all throughout
(4.) Neither Type I nor Type II, but a genre all its own
(5.) This may be Type I or Type II, but you cannot tell which one it is
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
I think #2 (i.e. 2AVB Type I)
I think #2 (i.e. 2AVB Type I) only because of the 3rd and 4th complexes. Otherwise, if given the strip I'd refer to it as 2:1 AVB, likely Type I due to narrow complexes.
Christopher
sixlettervariable.blogspot.com
ems12lead.com
I suspect this is an av block
I suspect this is an av block type 1 with variable conduction. However, I would be reluctant to treat my patient based on that in pre hospital due to inability to 100% rule out a type 2 with an escape complex based off of one strip. I would want to see a much longer run before I was confident.
All Mobitz I
Agree completely with Christopher. There is a regular atrial rate and 2nd degree AV block. The 3rd and 4th complexes clearly demonstrate Mobitz I (AV Wenckebach). The rest of the tracing shows 2nd degree with 2:1 AV conduction - but given the "context" - this is all Mobitz I because:
Excellent illustrative tracing by Jason.
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Looks like Mozitz I
Looks like Mozitz I (Wenkebach) with both 3:2 and 2:1 conduction. Althought technically you can't tell the difference between Mobitz I and Mobitz 2 when you only have a 2:1 conduction, "the company it keps" (ie the 3:2 conduction) allows us to determine this is Mobitz I and not Mobitz 2.
Sarah
I think is a type III block
I think is a type III block AV with a high idioventricular rhythm.
Semantics
We're really dealing with a question of semantics up to a point. It's a second degree AV block throughout, starting and ending with 2:1 conduction ratio (which could be either Type I or II) and with a Type 1, 3:2 conduction ratio in the middle. I agree with Sarah. If I had to choose, I would say it's a Type I switching from 2:1 to 3:2 and back based on the company it keeps. But although it seems unlikely, isn't it also possible that it is changing from a Type II to Type I and back again and that this is the reason the conduction ratio changes?
Walter A. Mueller, CCT, CRAT
WPW
I agree with averroes. I also think it's WPW
Caprice Hill Black
IMHO - I'll go with answer # 1 - 2nd deg AV Block, Type I & II
The ECG tracing starts with a Mobitz II with 2:1 conduction (Two P waves to one QRS complex), then in the middle of the tracing, the PR interval progressively gets longer and longer until a QRS is blocked, converting to a Mobitz I with a 3:1 conduction-Wenckebach (Three P waves to one QRS complex), then the tracing ends converting back into a Mobitz II with a 2:1 conduction (Two P waves to One QRS complex).
INTERPRETATION
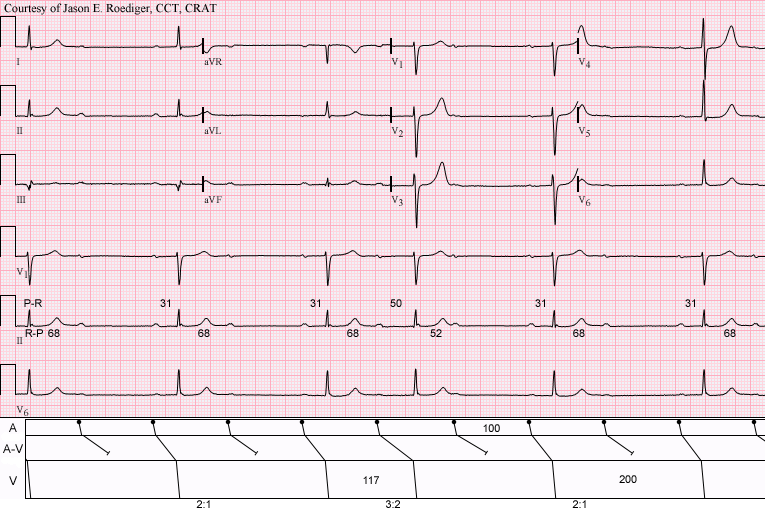
INTERPRETATION:(1.) Sinus rhythm (rate = 60/min) with Type I A-V block manifest in the form of . . .
(2.) . . . 2:1 A-V block and a . . .
(3.) . . . 3:2 Wenckebach period
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Type I Block
Thanks, everyone, for your answers, and to Jason for presenting this interesting ECG. It is not expected to "switch" from Type I to Type II, and it is not just "semantics". Type I blocks occur in the AV node and tend to be benign, while Type II blocks occur below the AV node, usually in the fascicles, and are decidedly NOT benign. It is important to determine which one you are dealing with. 2:1 conduction can make it difficult to make this determination, so when you have a period of 3:2 conduction, it is a GIFT, and it allows you to see what you are actually dealing with. Other clues are: wide QRS favors the diagnosis of Type II block, non-conducted P waves outside the refractory period of the ventricles favors Type II. Dr. Ken Grauer and Christopher Watford's comments above should be noted!
Dawn Altman, Admin