
Submitted by jer5150 on Sat, 02/09/2013 - 17:59
Patient's clinical data: 84-year-old black man
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
mobitz type 1 with prolonged qtc
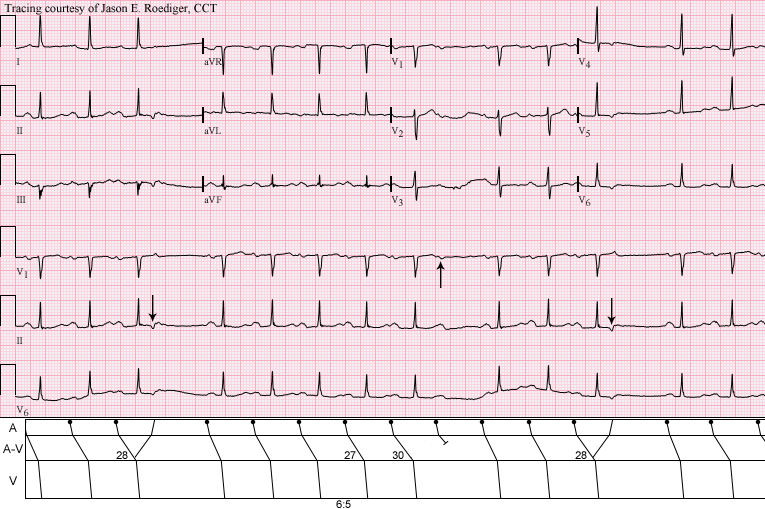
1. Atrial rate: 96 bpm, ventricular rate: 78 bpm
2. Sinus rhythm, irregular, in 'clusters' of beats
3. Axis normal
4. PR interval prolongation with subsequent non-conducting p waves (4th, 10th, 14th beat) = second degree heart block, Mobitz type 1 (wenkebach type)
5. 'Camel hump' T wave as a result of PR prolongation causing p to fuse with T waves.
6. QRS interval normal
7. QTc = 0.465ms = ?long QT for a man
8. No high voltage to suggest ventricular hypertrophy, no ischemic ST-T changes, no evidence of past MI
My impression: Sinus rhythm (sinus rate of 96bpm) and ventricular rate of 78bpm complicated by second degree Mobitz type 1 AV block with prolonged QTc
would want to check for:
hypomagnesemia
hypokalemia
hypocalcemia
drugs eg antiarrythmics, TCA, antipsychotics
Hope to learn his clinical condition from you. Thank you for sharing!
echo/reciprocal atrial beats
Nice, detailed description by jhwan. I would add one thing: the cause for the irregularity of the rhythm seems to be both the 2nd deg AVB type I (beat 10) and the non conducted atrial echo beats (beats 4 & 14 with their inverted P' waves). The Wenckebach is actualy the reason for the appeareance of these echo beats (when the AV conduction is prolonged enough, the VA conduction becomes possible and manifest; with a normal AV conduction duration, the VA conduction would probably remain concealed). A nice laddergram would nicely illustrate what happens in this beautiful ecg
Thank you
Thank you so much for your input. Learnt something interesting from you :)
Gorgeous Example of Mobitz I with Echo Beat Termination
First - GORGEOUS tracing by Jason!
THANKS for presenting Jason!
Ken Grauer, MD www.kg-ekgpress.com [email protected]
INTERPRETATION
INTERPRETATION:
(1.) Sinus rhythm (rate about 98/min) with . . .
(2.) . . . Type I A-V block manifest as a . . .
(3.) . . . 6:5 Wenckebach period.
(4.) Two probable reversed reciprocal beats (i.e., atrial "echos" - see laddergram).
COMMENTS:
It's important to remember that delayed conduction favors reentry. While this is certainly true, it is also important to realize that the conditions need to be just right. Twice we see a potential for Wenckebach periodicity as evidenced by the progressively lengthening P-R intervals and twice this progression is interrupted by retrograde P'-waves (downward arrow) in lead II. I would postulate that these represent atrial "echos" because they both follow identically prolonged P-R intervals of 0.28s. Then why isn't an atrial "echo" responsible for the pause in the middle of the tracing? Again, I would postulate that if the P-R interval is 0.27s, it is too short for reentry to take place. Conversely, if the P-R interval is 0.30s, it is too long for reentry to take place. In other words, there is a very narrow "window of opportunity" or one could say the "Goldilocks zone" required for reentry to take place is exactly 0.28s. If the prolonged P-R interval is any shorter, reentry doesn't occur. If the P-R interval is 0.30, it won't occur either. Any longer than 0.30s, and the next descending sinus impulse arrives at the A-V node during it's absolute refractory period and results in a "dropped" beat (upward arrow in lead V1). If all I saw in this ECG were pauses generated by atrial "echos" and the absence of any "dropped" beats, then I would not call this pure Type I A-V block. I would simply state that there was a "potential" for Type I A-V block. Case and point, if you refer to this ECG of a "Floating P-R interval", you will notice the the length of the P-R interval is waxing and waning. There are times when the P-R interval is progressively lengthening but does not result in the "dropped" beat. Instead the P-R interval retreats back to a shorter duration. As is, one can't assume that the patient's rhythm will ever progress to "dropping" beats until there is direct evidence that it does so.
Nonconducted APBs can't be completely ruled out, but as Ken pointed out, atrial "echos" are for more likely given the "company that it keeps" - that being, the 6:5 Wenckebach period.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Constructing a laddergram
-
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]