
Submitted by jer5150 on Tue, 08/06/2013 - 19:25
Patient of unknown age and gender with a history of atrial fibrillation. What's your interpretation?
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Nice EKG
Mark Sinus-Bradicardia, Bk-PAC, 1 SVPB noted, LAD, Q Waves 1/L, Poss LAHB.
non-conducted atrial bigeminy?
I think there is an underlying sinus rhythm; rate can't be determined because there are not 2 consecutive sinus P waves. The 2nd beat appears to be an atrial premature beat with aberrant conduction. Thereafter I think there is a subtle premature P wave, with a different shape from the sinus P wave, after each T wave and as this P wave is not followed by a QRS, the rhythm can be decribed as non-conducted atrial bigeminy. The ECG is otherwise normal
Dave R
SB
Looks to me to be a straight out sinus bradycardia, rate 36bpm, with PAC (2nd beat), and (?) U waves demonstrating prolonged repolorisation. That said, the T - U wave may be hindering my ability to see smaller P waves morphologically different to the others, suggestive of Dave R's suggested interpretation of non conducted atrial bigeminy. I can't however see an indication of left axis deviation, nor a left anterior hemiblock as suggested by marionurse. QRS width normal, and good R wave progression in pre cordial leads.
I'd like to know how the patient reverted from AF. Is the history paroxysmal AF, with spontaneous reversion, or was chemical or electrical cardioversion performed? My guess would be this is post DCCV.
My conclusion: either SB, or non conducted atrial bigeminy with premature atrial contraction.
It looks to me like marked
It looks to me like marked sinus bradycardia, with and aerrantly conducted PJC, normal frontal axis with low voltage and counterclockwise R wave progression. It almost makes me think escape beat but I don't see much of a non-compensatory pause.
IVAN J NASH
Sinus bradycardia/aberrant PAC
I don't see any definite blocked/non-conducted P-waves so I would say this is sinus bradycardia with an aberrant PAC. I would like to see a rhythm strip on this one :0)
HOCM
Sinus bradycardia , one PAC with aberrant conduction , normal axis, tall R in V2-V3 and pathological Qs in I and V6, likely secondary to septal hypertrophy. I'd say HOCM.
Stay where you are, use what you have, do what you can...
A bigeminy
Nice ecg.
Looks like underlying sinus rhythm with atrial bigeminy( Decent looking PR segment length, otherwise a PJC). The first PAC is conducted but met with aberrant right bundle branch block, with the subsequent bigeminy beats experience full refractory of the av node. I would also think it's non compensatory pause in this case. Estee's criteria not suggestive of LVH.
KinCiong!
some fanciful extrapolation
I would love to see the 2 or 3 beats immediately preceding this strip. Let's suppose this is an atrial bigeminy and that those preceding beats would show the sinus rhythm. In other words, the atrial bigeminy starts with the aberrated PAC. Then we could demonstrate to our students that the reason for the switch from an aberrated PAC to non-conducted PAC's is due to a greater degree of physiological block in the long-short cycle (Ashman's Phenomenon). The R-R interval after the aberrated beat would be the long cycle (when compared to our imagined sinus rhythm R-R's preceding it) and the non-conducted P would be the short cycle following the long cycle.
Please excuse my flight of fancy. Just in that kind of mood today. :)
Walter A. Mueller, CCT, CRAT
Atrial Bigeminy with Blocked PACs
I agree with David Richley's interpretation. This tracing is VERY subtle. A suggestion to increase size of the tracing - is if you print out a download or screen shot of the figure on an 8.5 X 11 piece of paper - then the tracing will be larger than it appears on the screen. This helps - given the ever-so-tiny but yet real amplitude of the blocked PACs ...
NICE tracing!
Ken Grauer, MD www.kg-ekgpress.com [email protected]
Sinus bradycardia with non conducted PAC
The rhythm shows bigeminy with one PAC embedded at the end of T wave after every beat
The first PAC is conducted aberrantly due to the above mentioned longer coupling interval by the PAC ( although i couldnt really tell it because the difference is really small ).
Ryan
Sinus bradycardia with non conducted PAC
The rhythm shows bigeminy with one PAC embedded at the end of T wave after every beat
The first PAC is conducted aberrantly due to the above mentioned longer coupling interval by the PAC, Here i uploaded a laddergram i did myself to illustrate this. Please give any opinions thanks !!!
https://www.dropbox.com/s/p8lnd65kjq62bpc/ECG%20of%20the%20Month%202q%20-%20Copy.jpg
Ryan
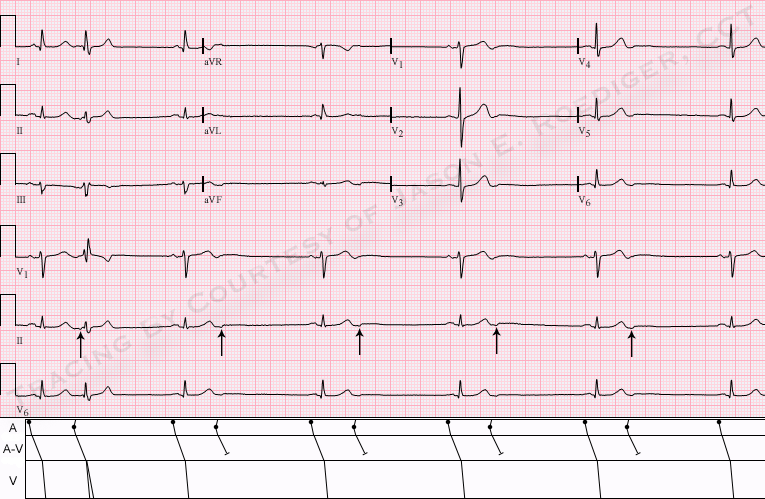
INTERPRETATION
INTERPRETATION:(1.) Sinus bradycardia (rate indeterminate) with mostly . . .
(2.) . . . nonconducted atrial bigeminy reducing the ventricular rate to about 36/min.
(3.) One atrial premature beat (APB) with right bundle-branch block (RBBB) aberrancy (2nd beat).
COMMENTS:
At a superficial glance, this ECG might be misinterpreted as a marked sinus bradycardia with one interpolated ventricular premature beat (VPB) or even an interpolated junctional premature beat (JPB) with RBBB aberrancy. The second beat’s QRS morphology is consistent in every way with the classical shape of RBBB with its triphasic rsR’ (i.e., “M-shape") in lead V1. There is also a triphasic qRs in leads I and V6 as well. The early ectopic atrial P’-waves (arrows) are very subtle and best seen in lead II. Ryan makes an outstanding observation about the slightly longer coupling interval on the first APB which is certainly contributing to whether or not the APB conducts aberrantly or not at all. Additionally, he has superbly diagrammed his findings here:
https://www.dropbox.com/s/p8lnd65kjq62bpc/ECG%20of%20the%20Month%202q%20-%20Copy.jpg
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]
Test Subject from app
Test