
Submitted by jer5150 on Sun, 03/30/2014 - 18:18
Patient data: 62-year old man.
Rate this content:
-

- jer5150's blog
- Log in or register to post comments
All our content is FREE & COPYRIGHT FREE for non-commercial use
Please be courteous and leave any watermark or author attribution on content you reproduce.
Comments
Pacer
I believe Sinus 1st degree av blk, INF changes and pacemaker L side, maybe VVI not the Best at pacers.
LV pacing?
This looks like a profound sinus bradycardia, atrial rate just under 30bpm, with VVI pacing at 65bpm. Unusually, there seems to be LV, rather than RV, pacing. The two narrow QRS complexes (beats 4 and 9) are conducted sinus beats: they each follow a P wave in the T wave of the preceding beat. There are also P waves before three of the paced QRS complexes (beats 2, 7 and 12) and these would almost certainly have conducted had the pacemaker not intervened first. Jason’s ECGs are usually fiendishly difficult and complicated so I fear I may have missed something!
Dave R
RV pacing
RV pacing with Junctional beats due to no P wave before 4, 9...
Hassan Alsafi
AV dissociation by paced default
- Severe sinus bradycardia @ approx 30 bpm
- LV(?) paced rhythm @ approx 49 bpm
- AV-dissociation by default
- #4 and 9 are capture beats
- #2, 7, and 12 are fusion beats
- RP/PR reciprocity as evidenced by the shorter PRi's on the fusion beats
- T-wave inversions of the supraventricular beats in V3-V6, II, III, and probably I and III, uncertain origin (coinsider cardiac memory if no other cause found).
- Poor R-wave progression of the supraventricular beats.
Vince D
http://www.medialapproach.com
Jason's ECG challenge April 2014
Probably a dual chambered Medtronic pacemaker that has reached Elective Replacement Indicator (BOL 85 ERI 65). Hook up to a programmer to confirm and schedule revision. Other possiblility would be a single chambered device that was previously set due to permanent Afib then converted back to sinus rhythm. Need more info on this patient, definitely need a programmer.
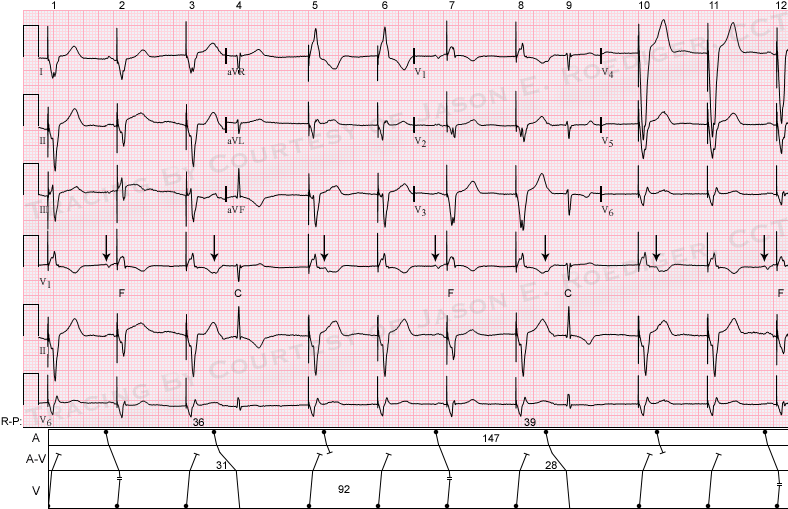
INTERPRETATION
INTERPRETATION:
(1.) Marked sinus bradycardia (rate about 41/min) dissociated from a . . .
(2.) . . . biventricular pacemaker (rate about 65/min) in demand mode (VVI).
(3.) Two ventricular capture beats (4th and 9th beats) with prolonged P-R intervals due to . . .
(4.) . . . retrograde concealed conduction.
(5.) R-P/P-R reciprocity.
(6.) Three ventricular paced fusion beats (2nd, 7th, and 12th beats).
COMMENTS:
The pacemaker is recognized as biventricular (Bi-V) from the wholly-negative QS complex in lead I. As Vince pointed out, there is poor r-wave progression on the sinus beat in leads V1-3 and the nonspecific T-wave inversions could be due to persistent ventricular pacing. Based on the normal P-V intervals of the fusion beats, the patient's intrinsic P-R intervals are probably also normal during sinus rhythm.
Jason E. Roediger - Certified Cardiographic Technician (CCT)
[email protected]