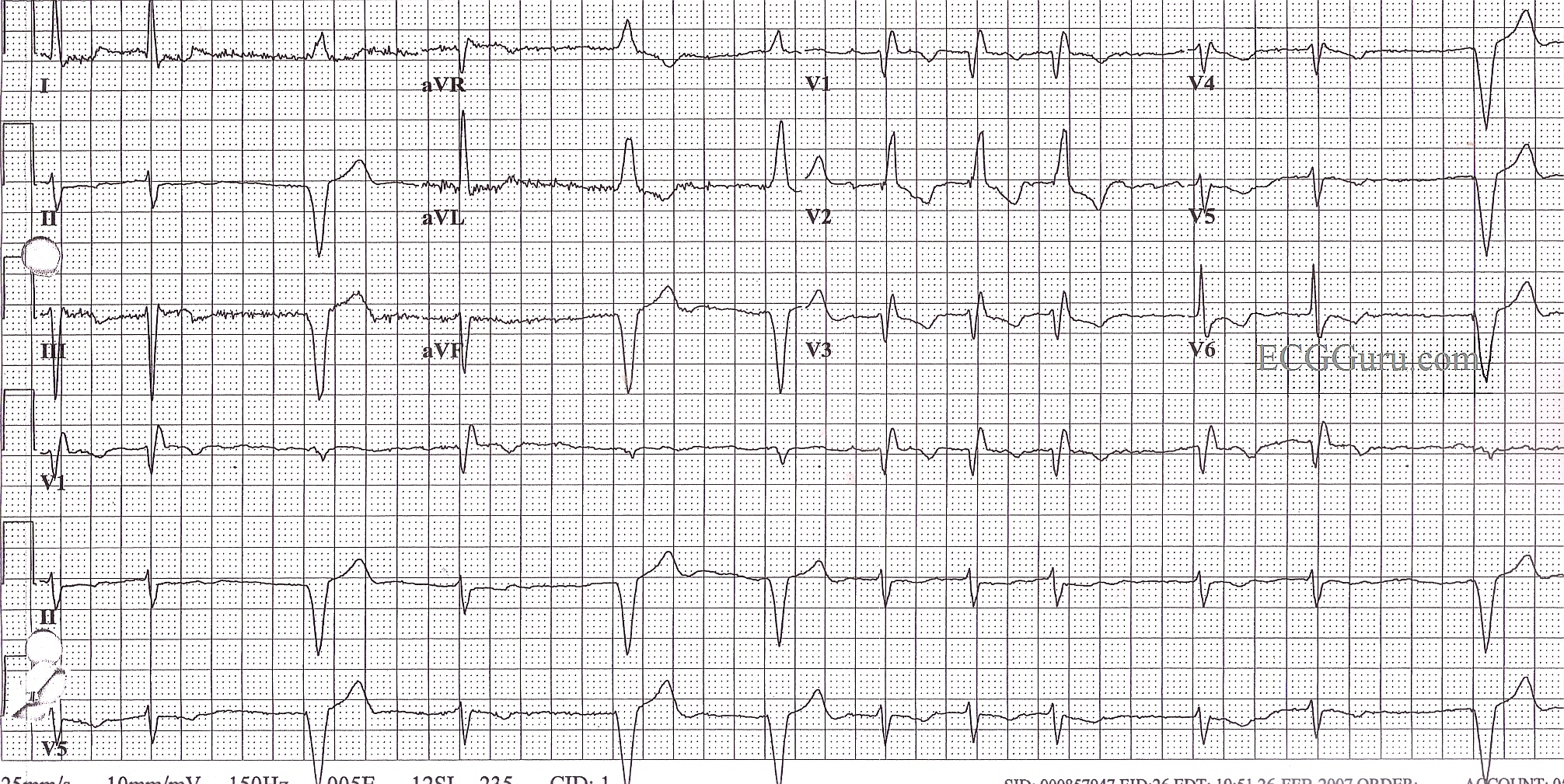
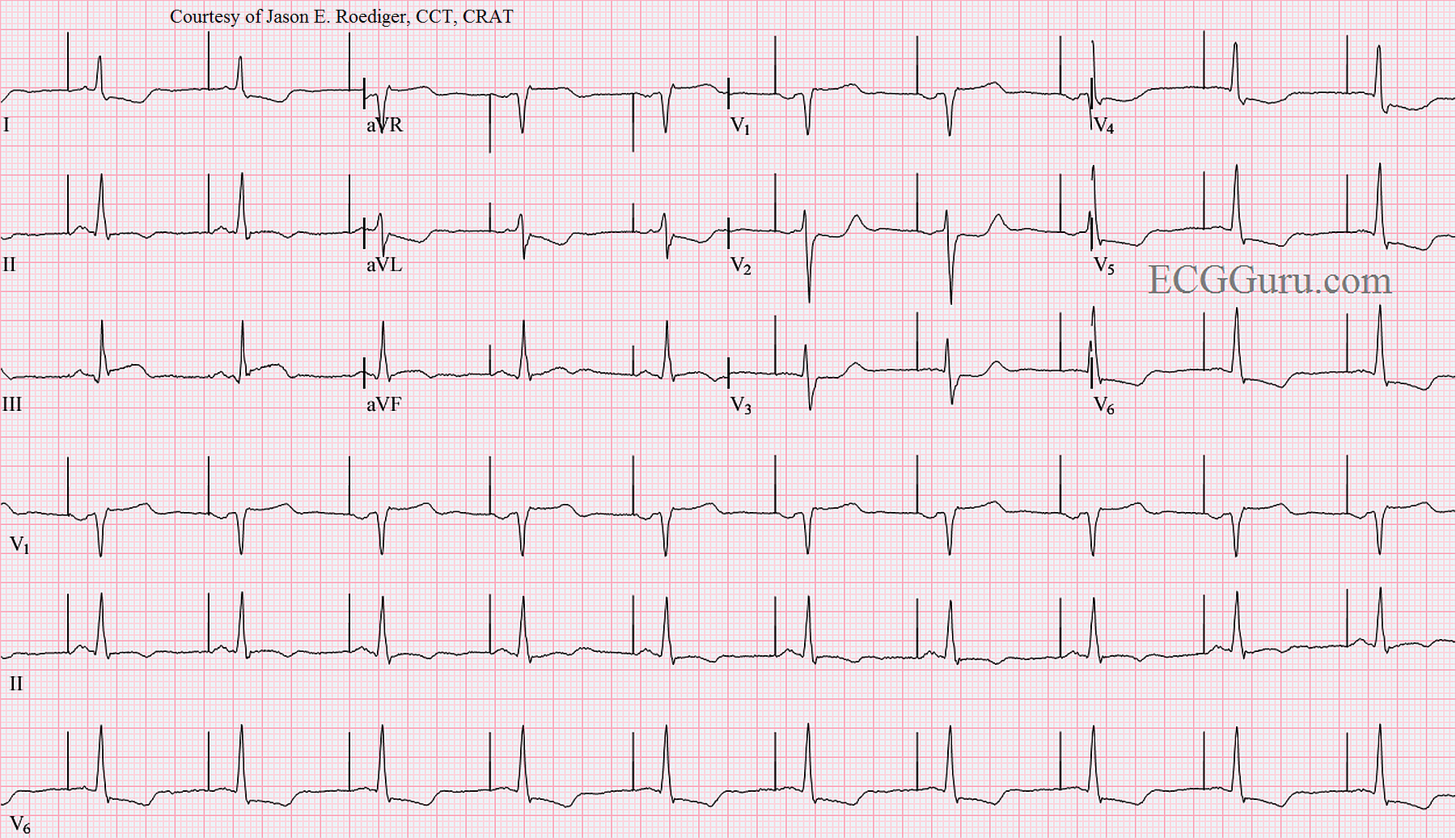
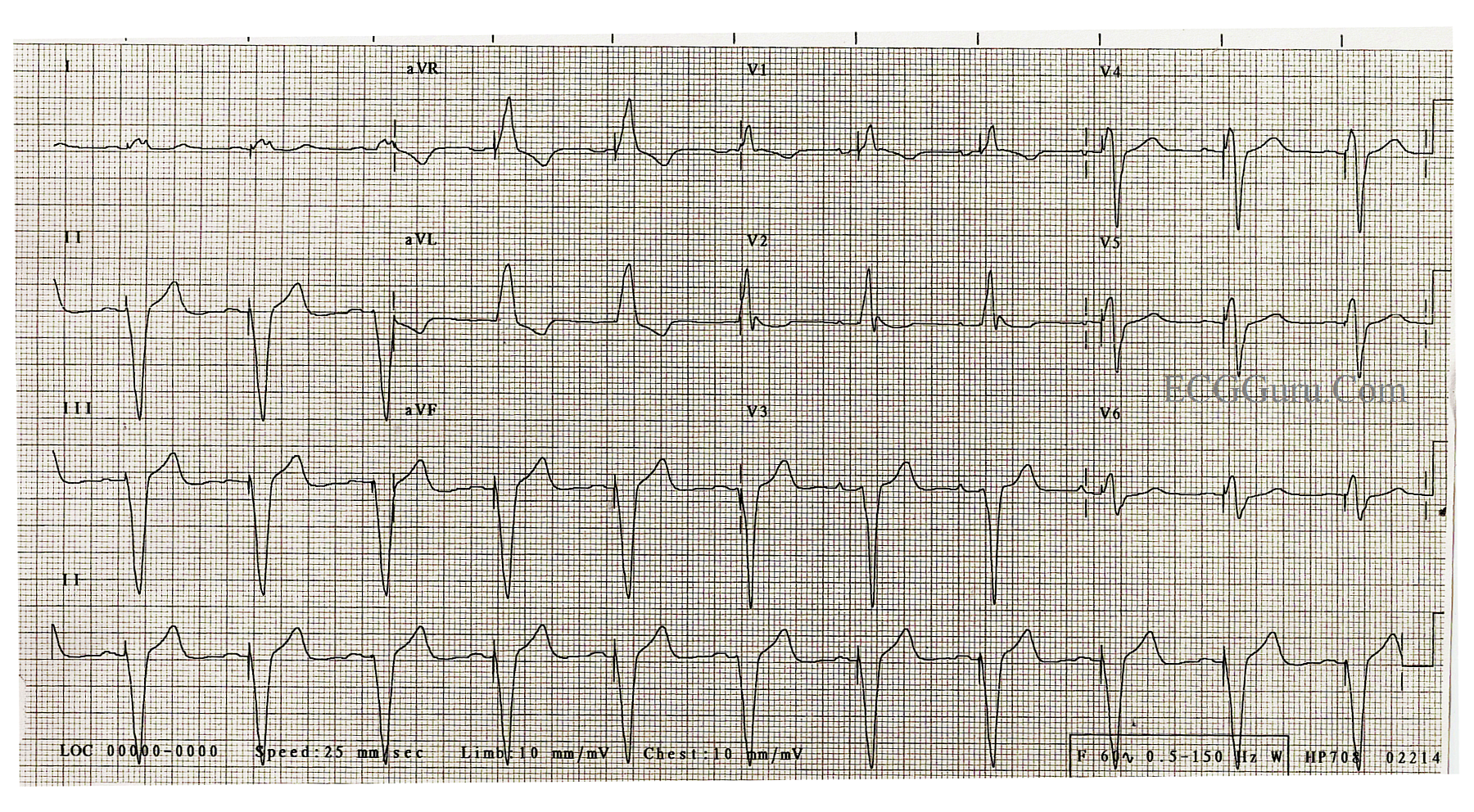
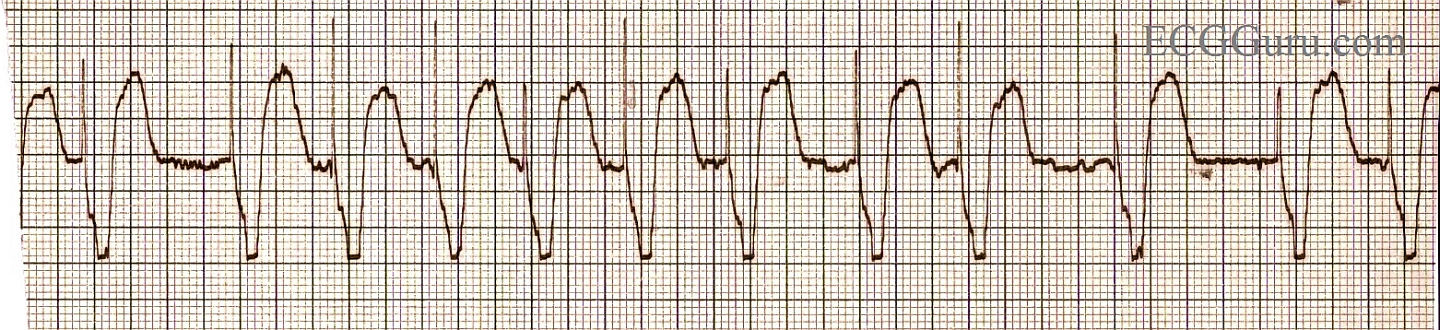
We caution students that the signs of acute M.I. (ST elevation) cannot reliably be seen in cases of wide QRS. This is because, in wide QRS situations like left bundle branch block, ventricular rhythms, or right ventricular pacing, the ST segments will elevate in leads with downward QRS complexes, and depress when the QRS is upright. These is called discordant ST changes.
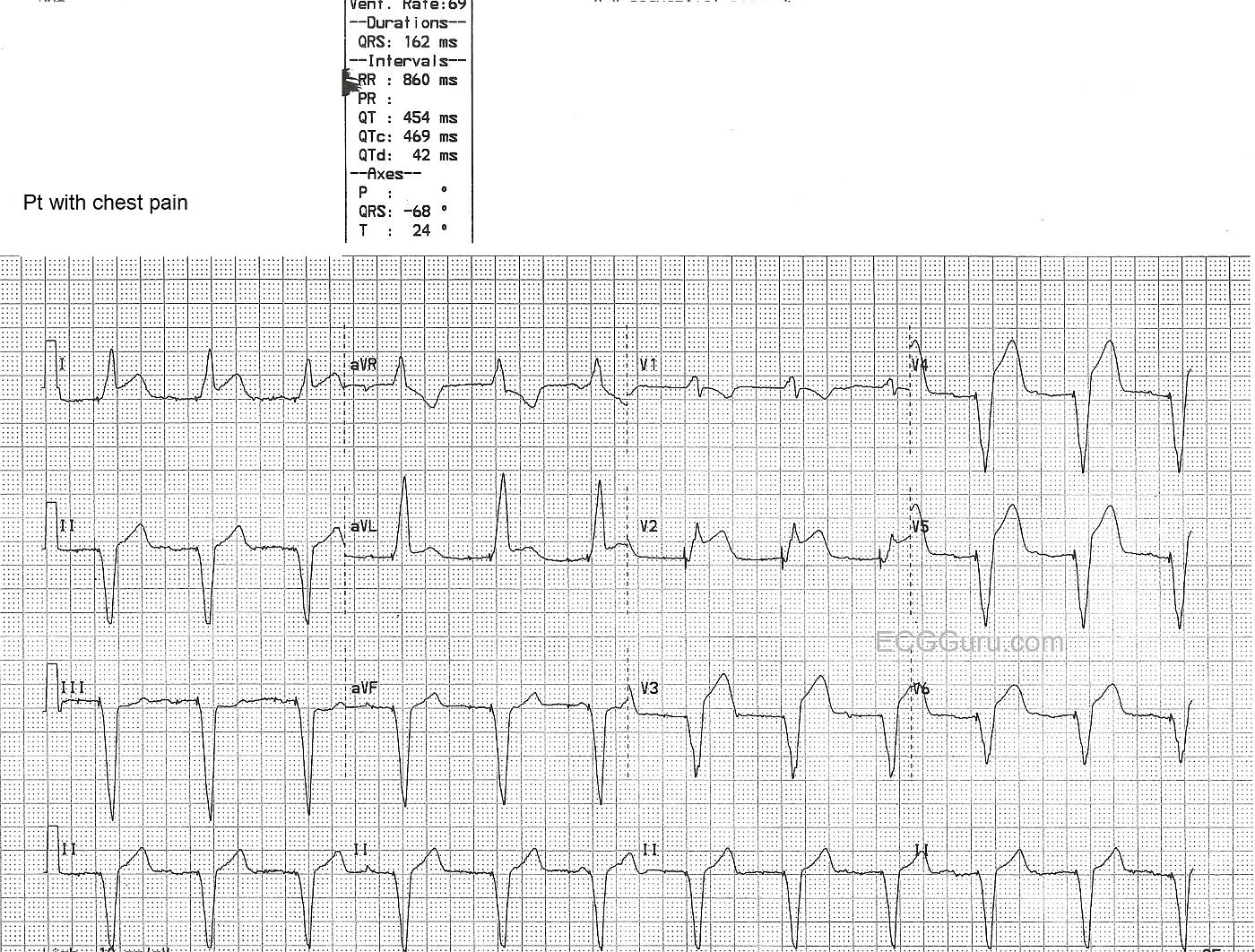
In this ECG, a man in his 60's presented with chest pain. His ECG showed AV sequential pacing, with ventricular pacing from the right ventricle. The QRS is 162 ms in duration. He has ST segment elevation in Leads I, aVL, and Leads V2 through V6.
The ST elevations are more pronounced than expected in this paced patient. But, the real clue here is the ST elevation in Leads I, aVL, and V2 - leads that should have ST depression because of their upright QRS complexes, have elevation! This patient was taken to the cath lab and the left coronary artery wass reperfused and stented. For more information about ST elevation in wide QRS complex rhythms, see this LINK.



 Do you ever feel confused by pacemaker rhythms? You are not alone! Pacemakers are electronic devices, and have rapidly evolved in their capabilities. Often, we call the manufacturer's representative to come and interrogate a patient's pacemaker to determine if it is behaving as it was programmed. Without knowing the programming of the individual pacemaker, it can be hard to evaluate the patient's rhythm.
Do you ever feel confused by pacemaker rhythms? You are not alone! Pacemakers are electronic devices, and have rapidly evolved in their capabilities. Often, we call the manufacturer's representative to come and interrogate a patient's pacemaker to determine if it is behaving as it was programmed. Without knowing the programming of the individual pacemaker, it can be hard to evaluate the patient's rhythm.