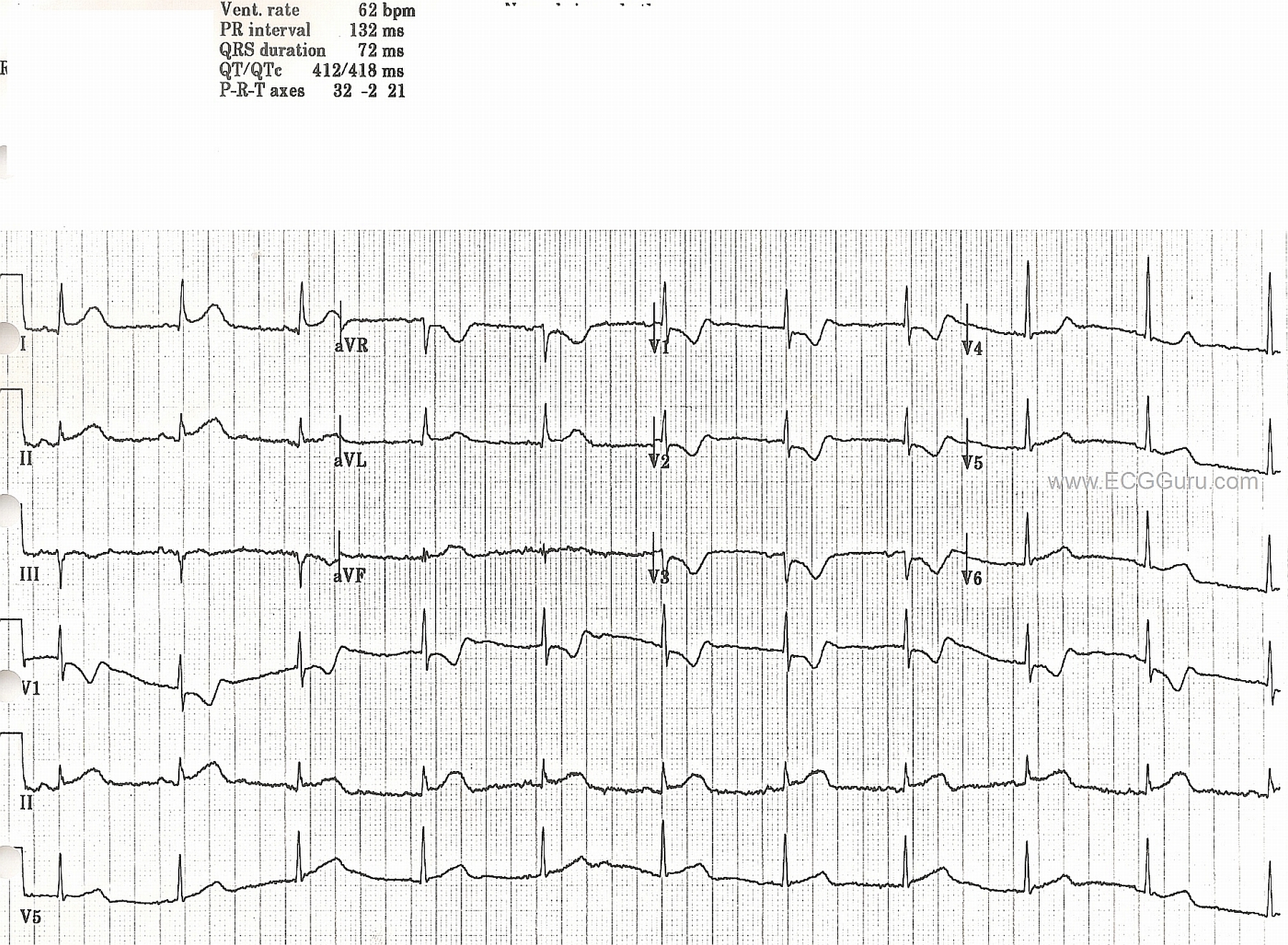
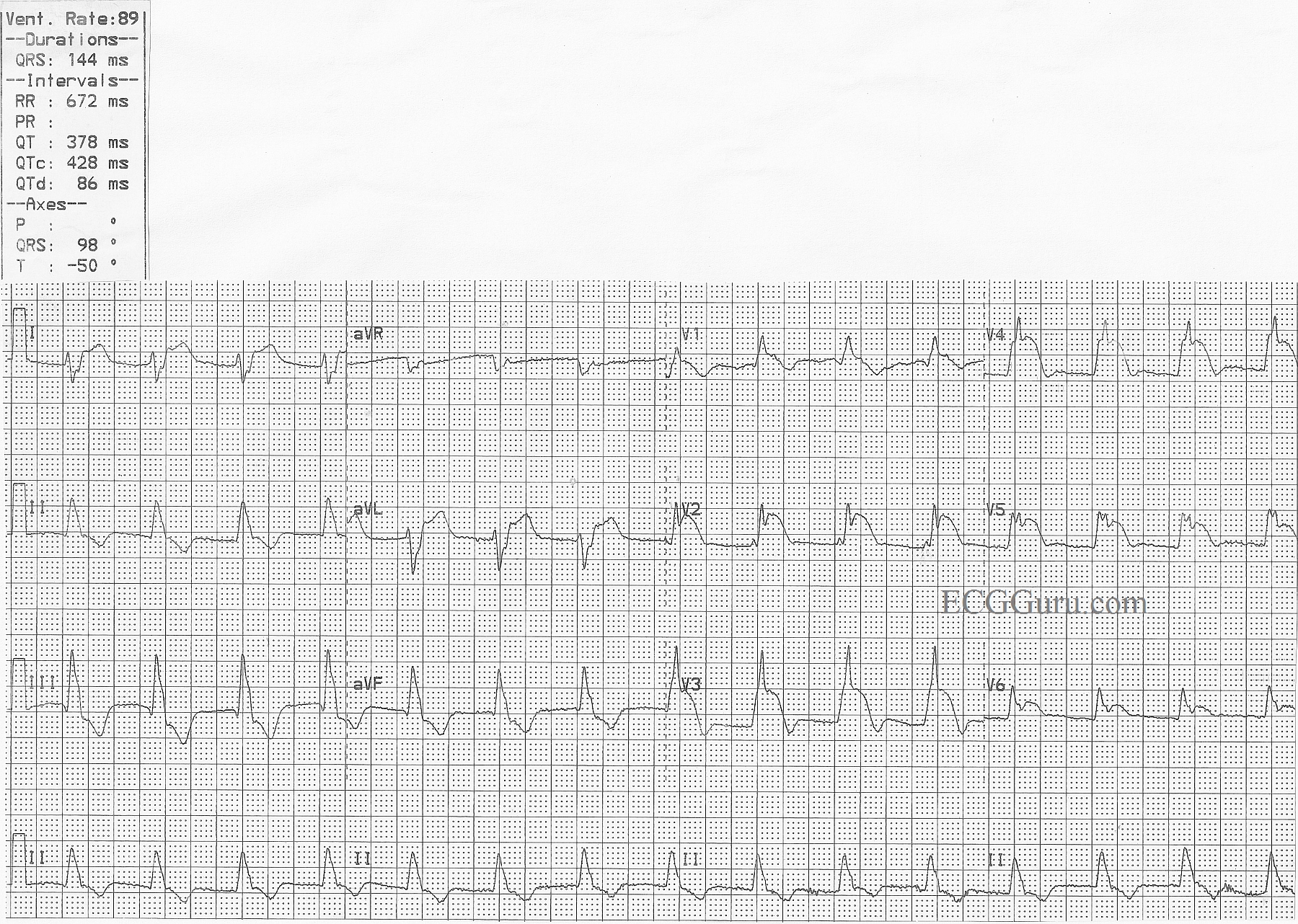
In this ECG, there is ST elevation in II, III, and aVF and reciprocal ST depression in I and aVL, indicating acute inferior wall M.I. Also, this patient has developed pathological Q waves in III and aVF, and probably II as well, indicating permanent damage to the myocardium. A ventriculogram or echocardiogram will confirm akinesis of the inferior wall in most cases. In this ECG, there is no ST depression in V1 through V3, so we can hope the posterior wall has been spared. Notice the flattening of the ST segments in the elevated leads. This is a sign of CAD. Last week's ECG had coved upward (frowning) ST segments, which are even more sinister looking. Lead V1 has the flattening, and a pathological Q wave. When V1 looks "sick" and V2 looks "well", there is a good probability of right ventricular injury as well. Lead III has a taller ST segment than Lead II. This has also been shown to be a marker of RVMI. Regardless, a right-sided ECG, or at least a V4 right, should be obtained in any IWMI, since the RCA often supplies both the right ventricle and the inferior wall of the left ventricle.
The rhythm in this ECG is interesting, as well. It appears to be sinus, but it is difficult to evaluate P waves. In the Lead II rhythm strip, they appear to change in morphology. Because the R to R interval remains constant, we feel this change in appearance is due to baseline artifact caused most likely by patient movement such as breathing. What do you think?
Our thanks to Andrew Porter for contributing this ECG.

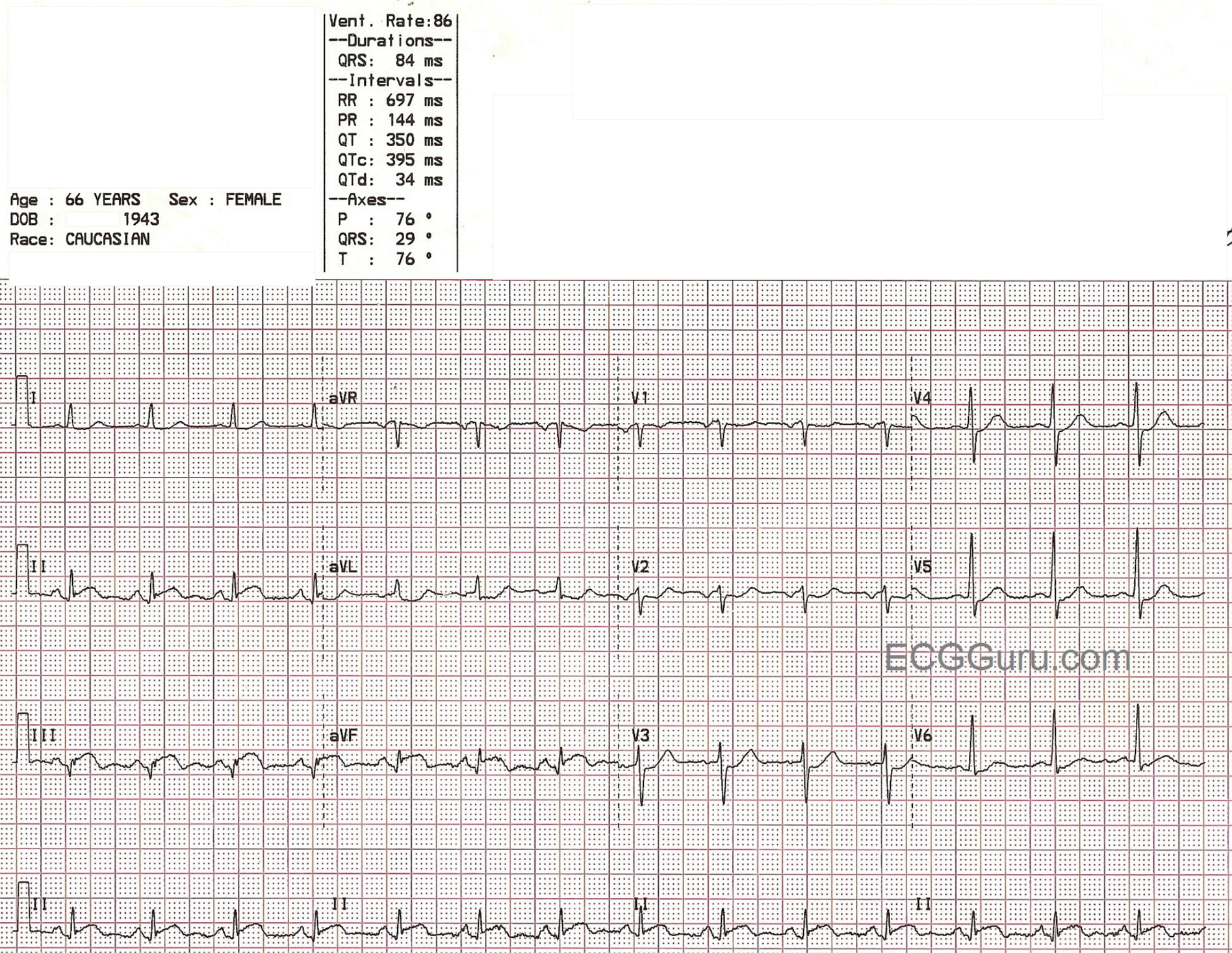

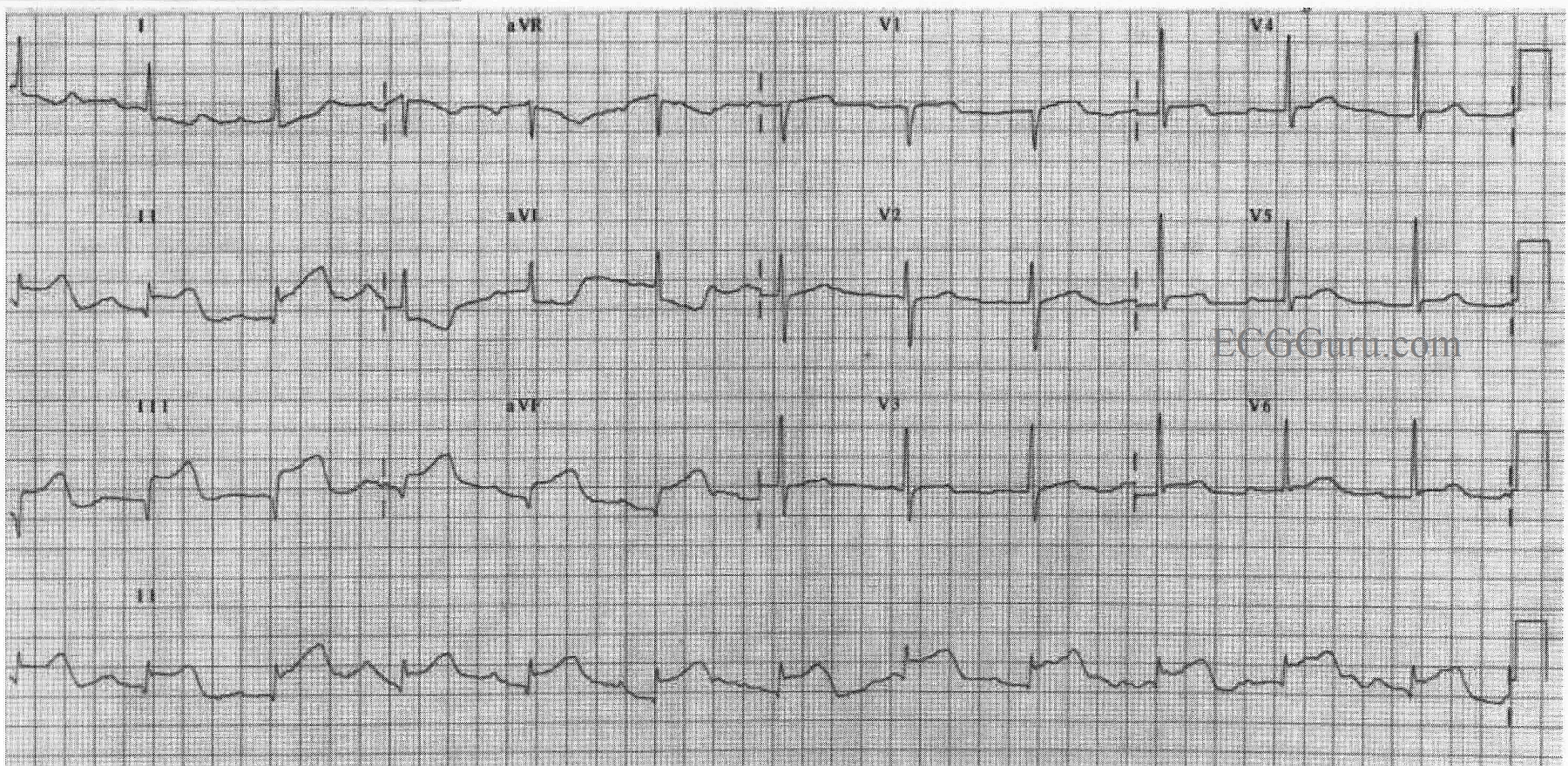
Many people with complete occlusion of the left main do not survive. When there is some diminished blood flow through the blocked area in the proximal LAD or left main, this pattern may appear. Look for ST elevation in aVR greater than or equal to 1 mm, ST elevation in aVR greater than the ST elevation in V1, and widespread ST depression.
In this ECG, aVR and V1 show ST segment elevation, with widespread ST depression. For years, aVR was virtually ignored in the literature, and considered to be only a reciprocal view of the lateral inferior wall. Now, there is convincing evidence of its usefulness in discovering proximal left coronary artery occlusion and severe triple vessel disease. ST elevation in aVR can be a reliable sign of ischemia of the basal part of the heart and the proximal IV septum.
Many people with complete occlusion of the left main do not survive. When there is diminished blood flow through the blocked area in the proximal LAD or left main, this pattern may appear. Look for ST elevation in aVR greater than or equal to 1 mm, ST elevation in aVR greater than the ST elevation in V1, and widespread ST depression.
For complete discussions on this topic, go to Life in the Fast Lane,
Dr. Smith's ECG Blog,
JACC