The Patient: 44-year-old man with chest pain. Symptoms started over 24 hours ago. The EMS crew recognized an acute M.I. on the ECG and transferred him immediately to a cardiac hospital. They started two I.V.s and gave aspirin enroute.
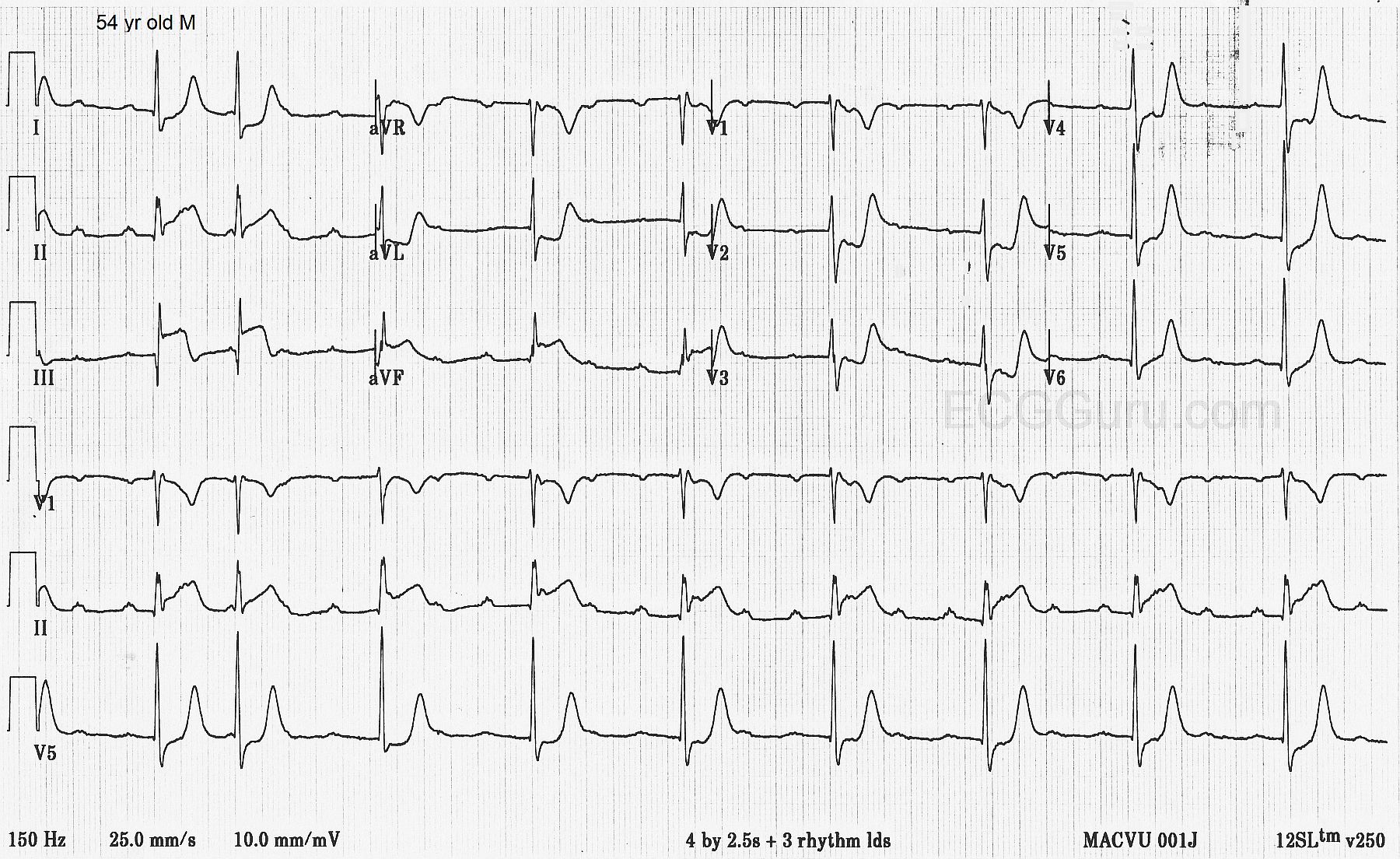
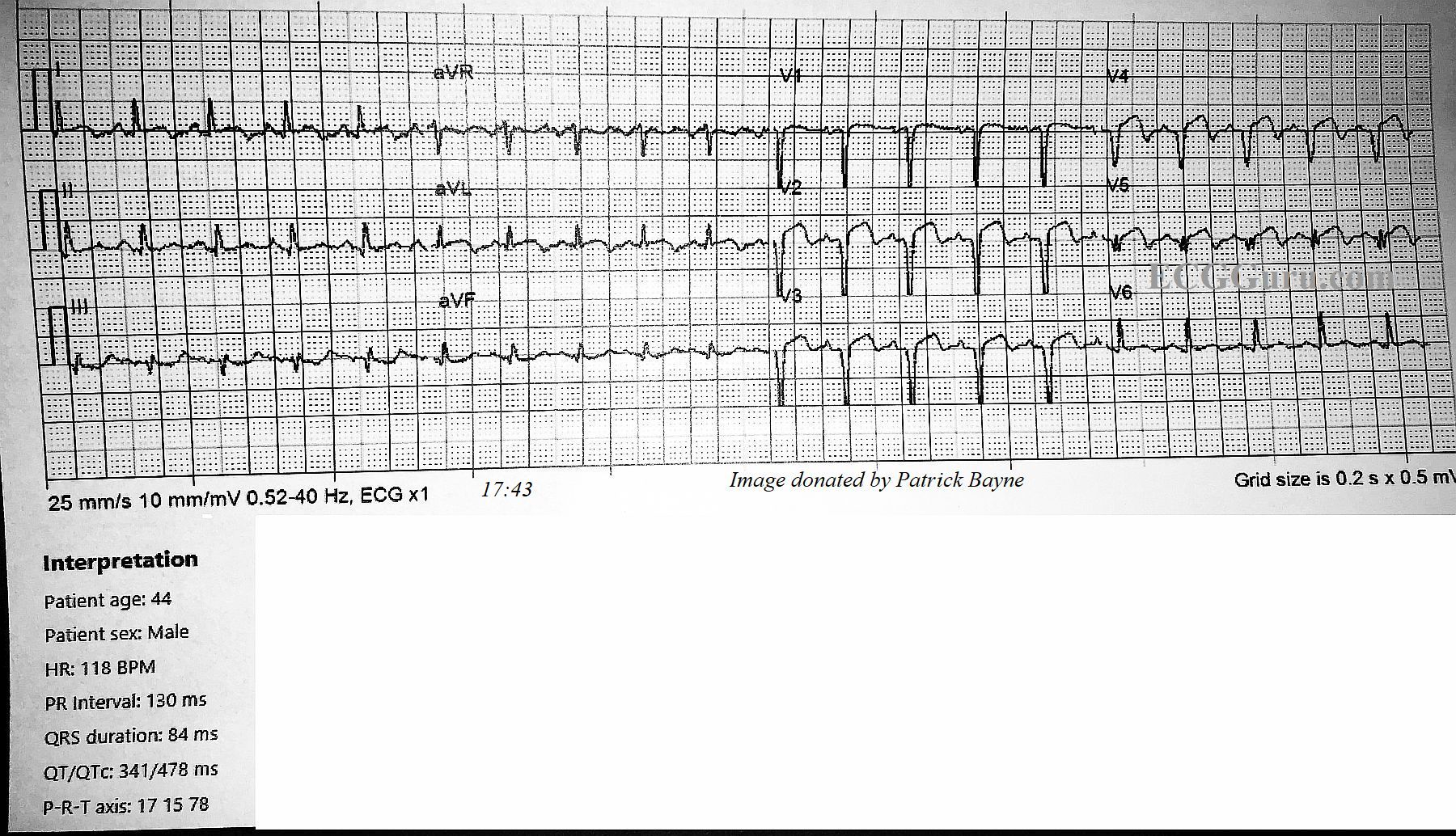
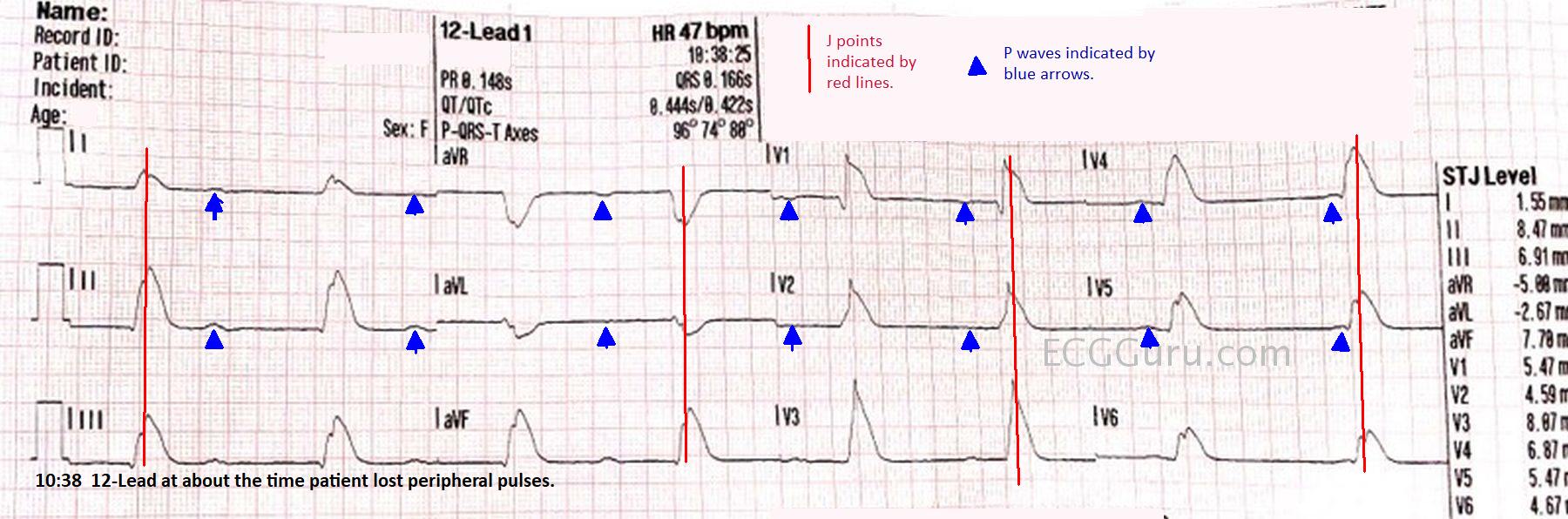
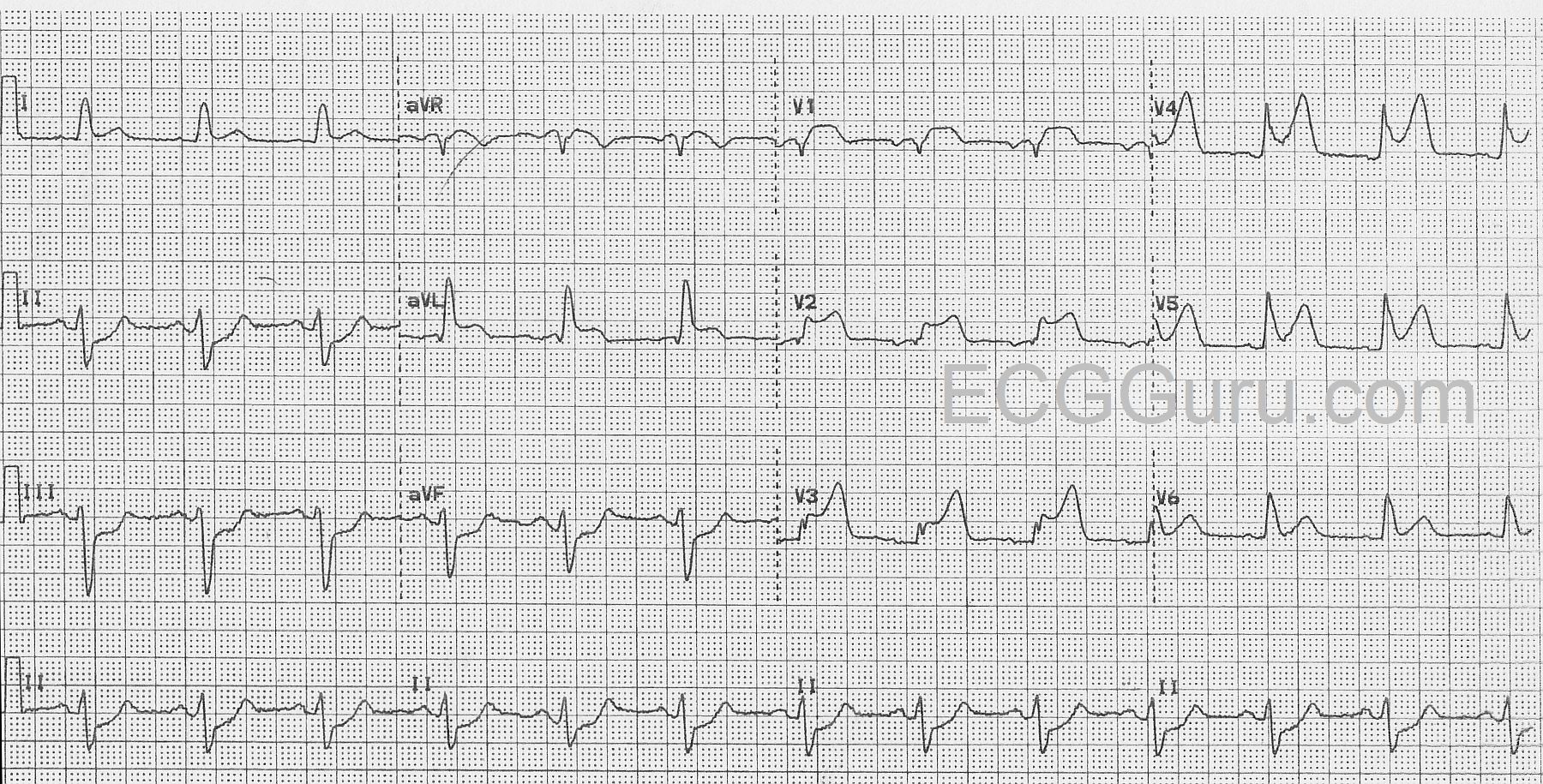
ECG No. 1 @17:43: The rhythm is sinus tachycardia at 118 bpm. The PR interval is within normal limits at 130 ms, and the QRS is narrow at 84 ms. The QTCc is 478 ms by the machine’s measurement, but we measured the QT at 303 ms and QTc as 376-419 ms via various methods, which are within normal limits. The QRS frontal plane axis is at 15 degrees, within normal limits.
The ST segments are elevated and mostly straight in Leads V1 through V5, I and aVL. There is mild ST depression in III and aVF. Very concerning are the pathological Q waves in V1 through V5, indicating loss (death) of myocardial tissue in the anterior wall.
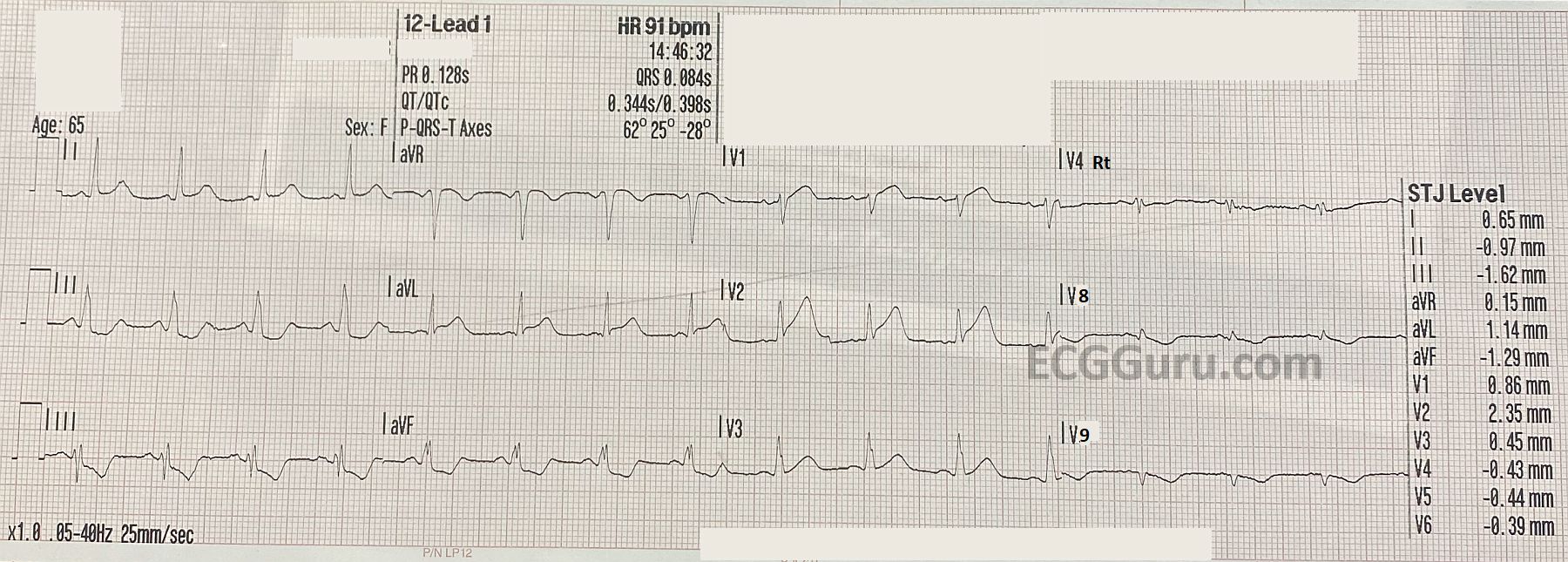
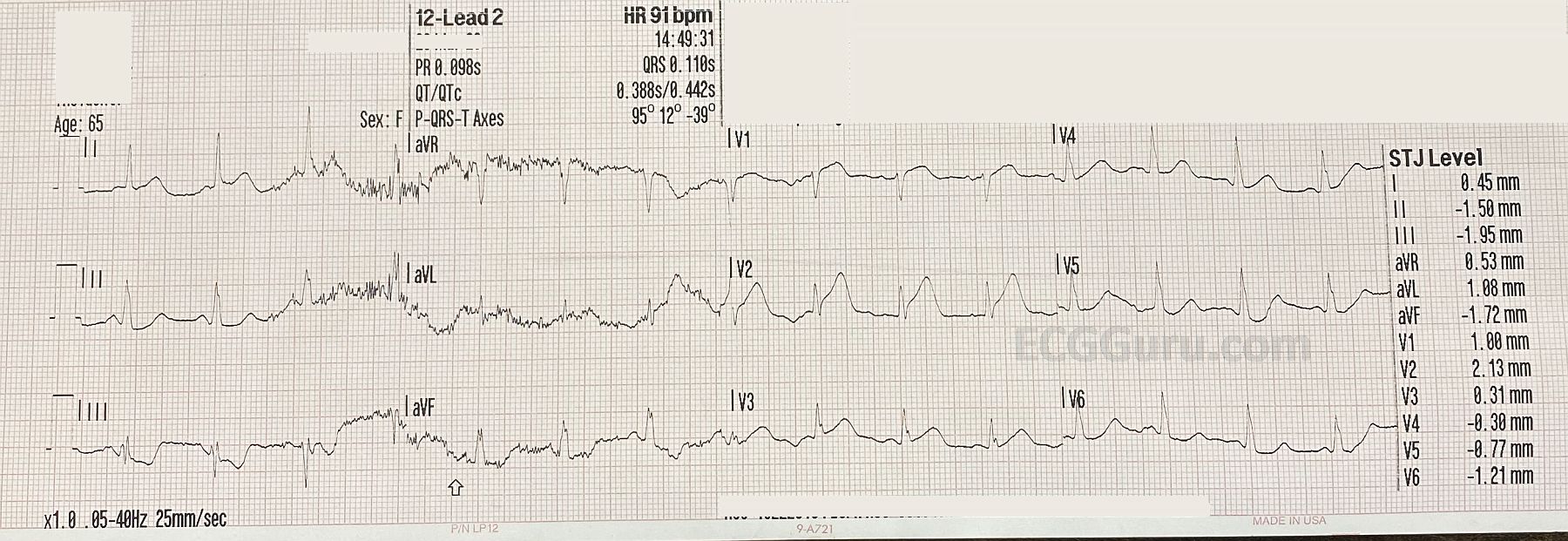
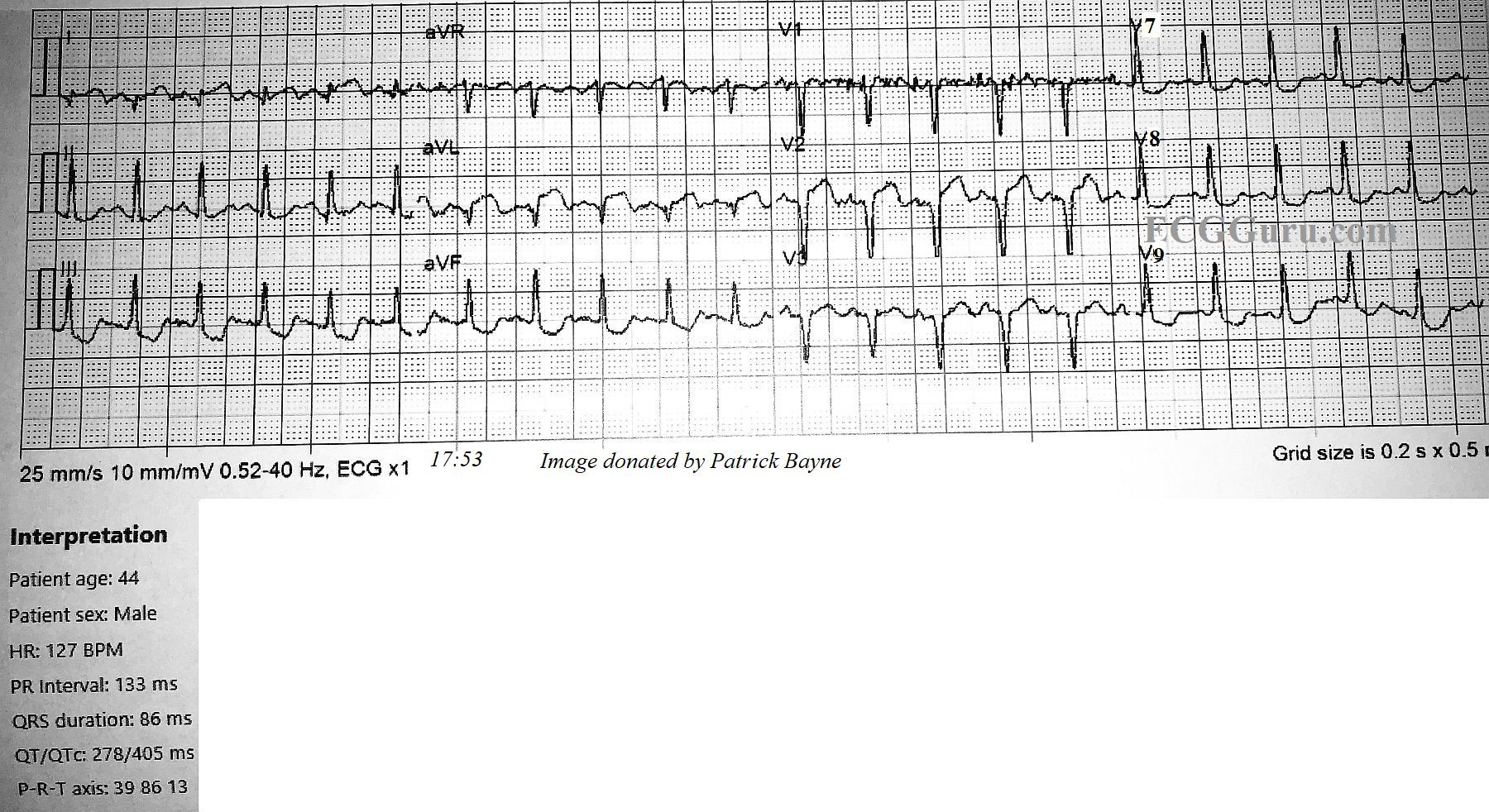
ECG No. 2 @ 17:53: The second ECG was performed about 10 minutes later, and V4, V5, and V6 were replaced by V7, V8, and V9. Reciprocal ST depression is observed in those additional leads. The heart rate is now 128 bpm. It is notable that pathological Q waves have now appeared in Leads I and aVL. There has been no change in lead placement. The onset of necrosis in the high lateral wall has shifted the frontal plane axis toward the right extreme of normal, at 86 degrees, and now II, III, and aVF have prominent R waves. Another cause for right axis shift in anterior wall M.I. to consider would be posterior hemiblock. However, that is a diagnosis of exclusion, and the new Q waves explain the axis shift. It is interesting that the onset of pathological Q waves was captured in these serial ECGs.