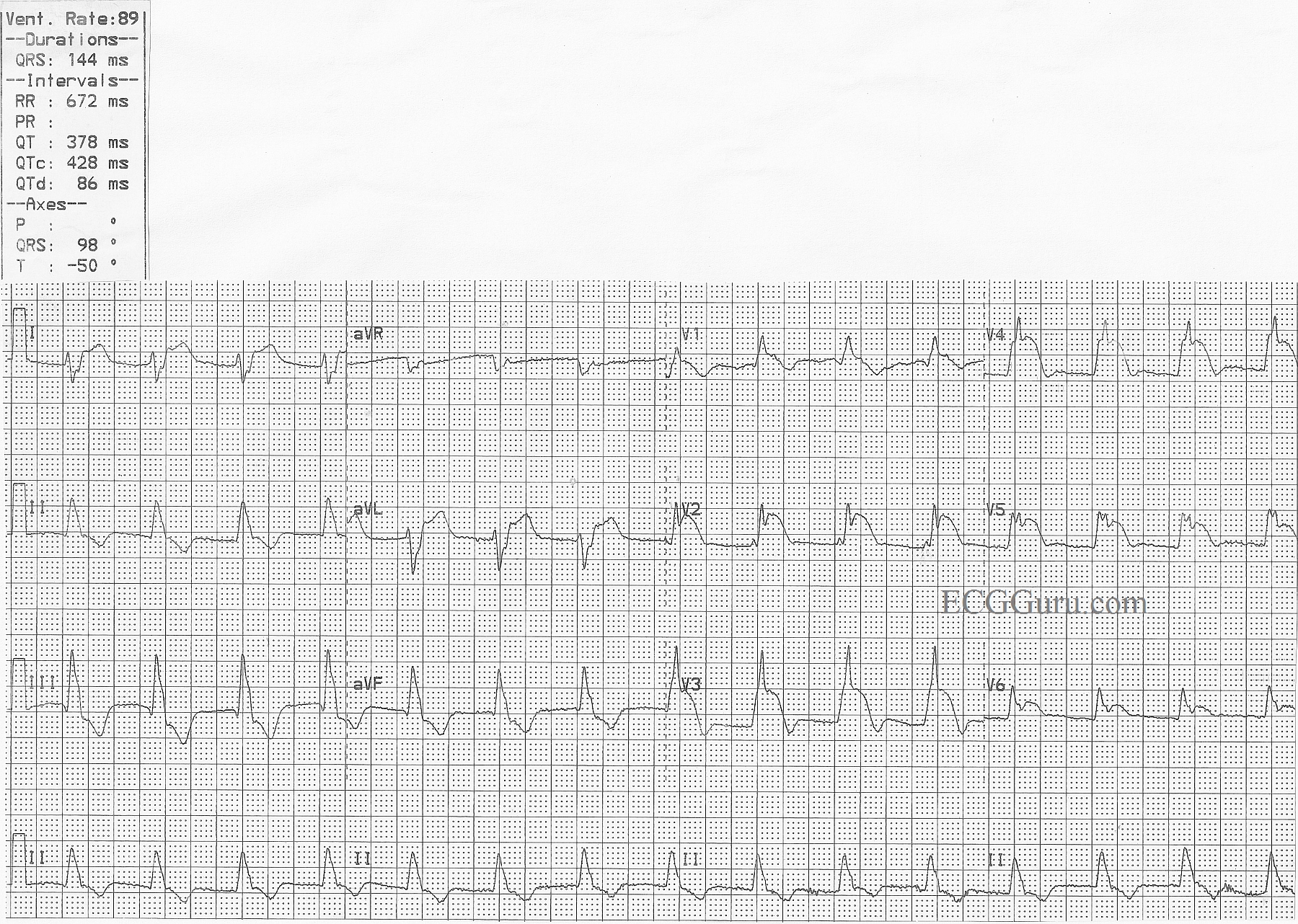
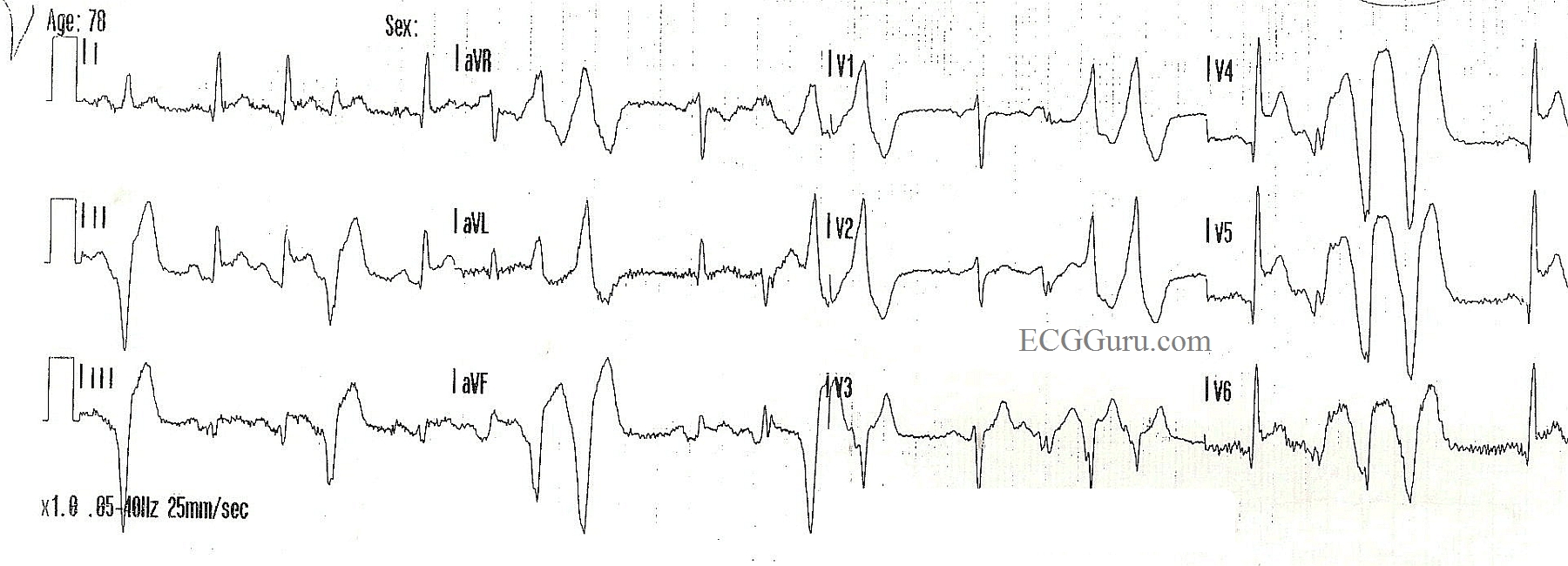
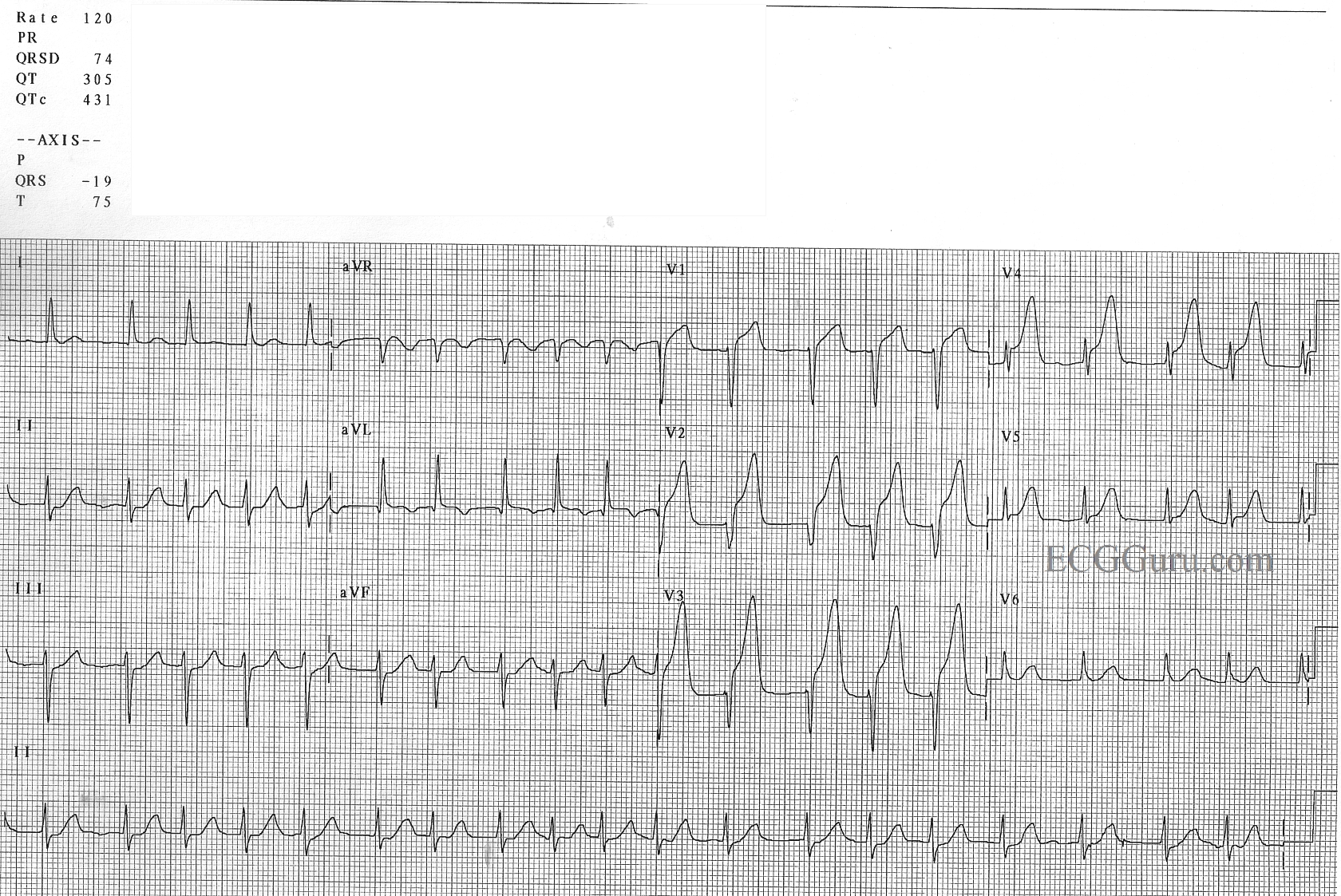
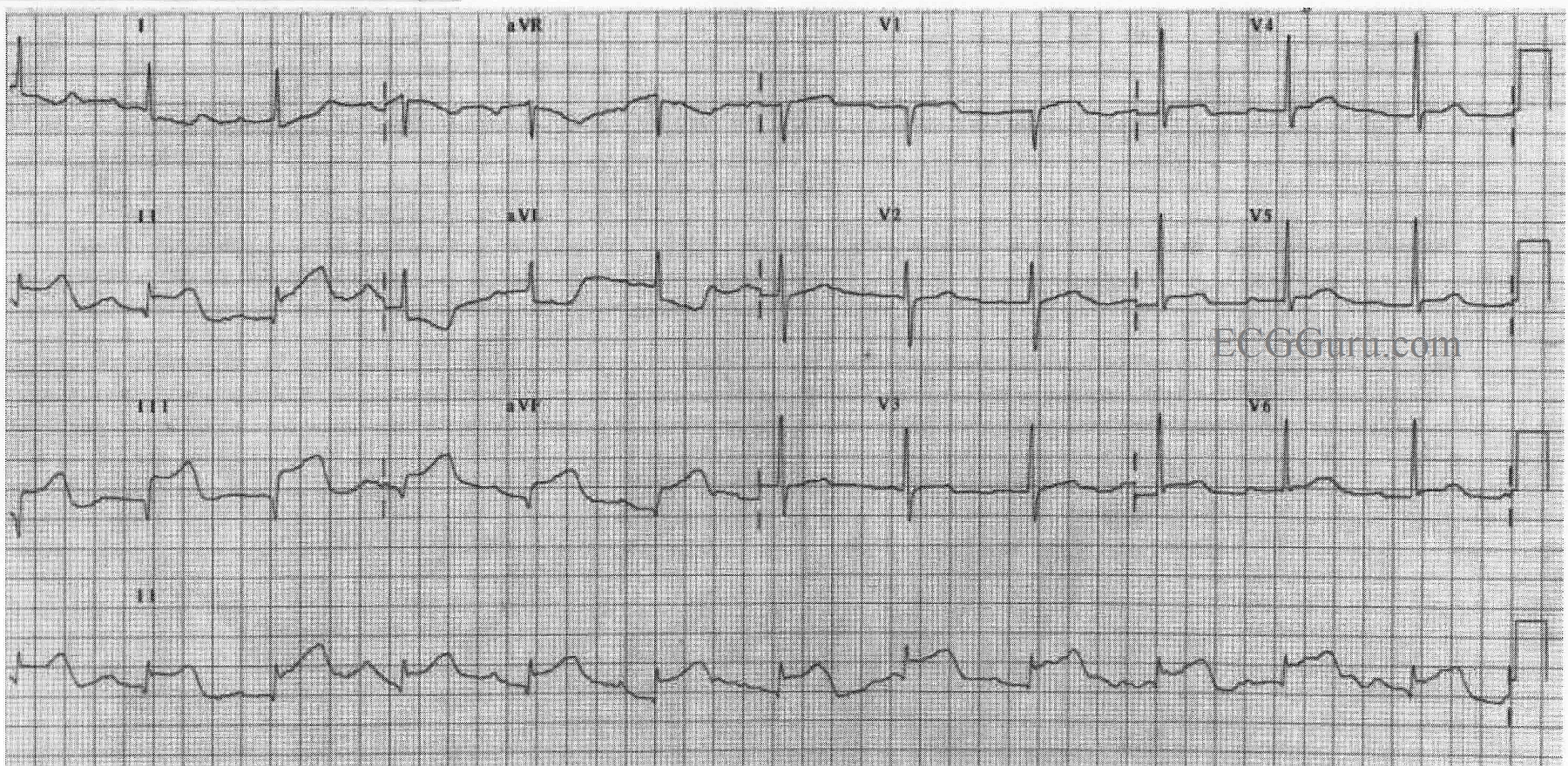
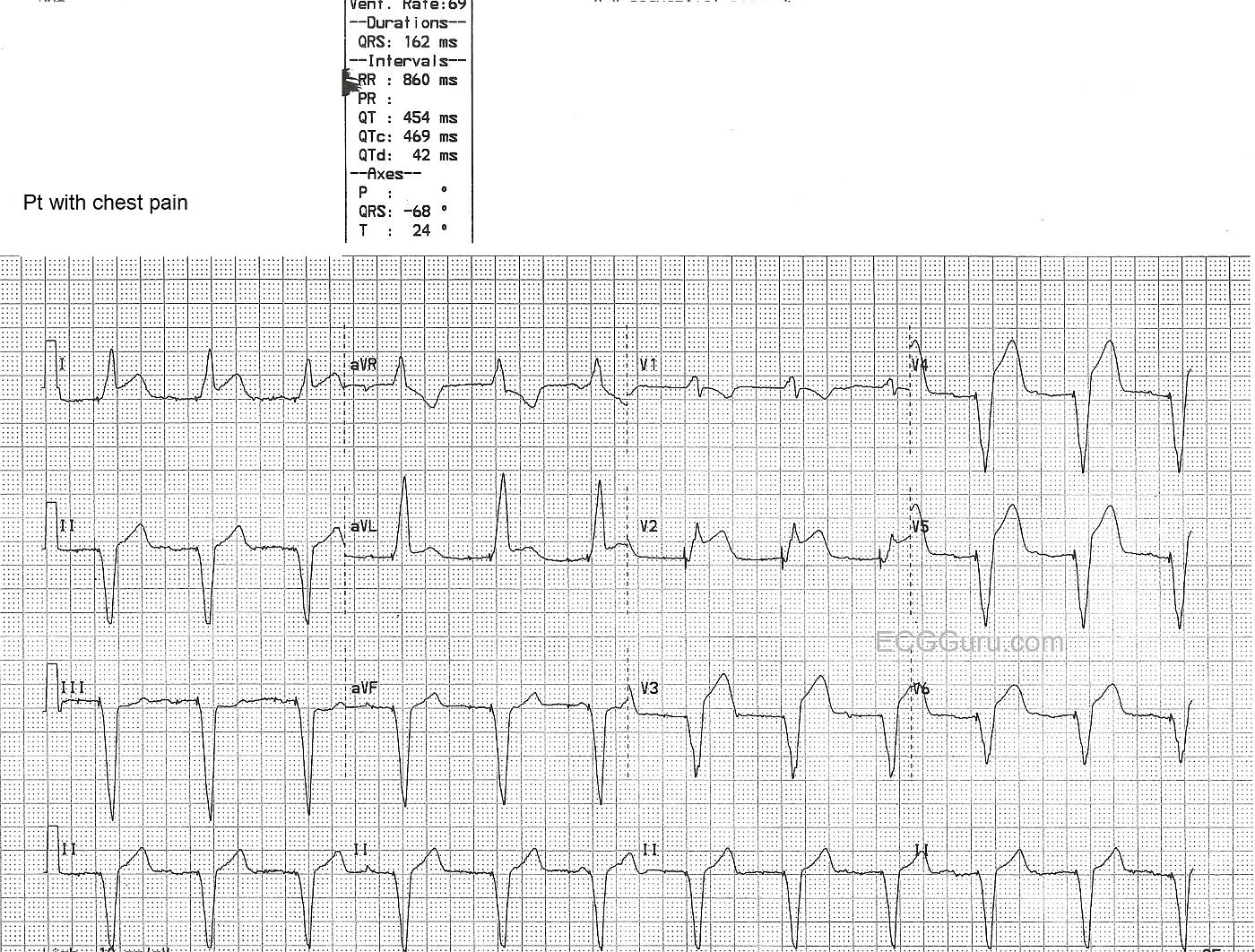
Patient AW103: This 88 year old woman had been sick for several days, but had not sought treatment. Her family found her nearly unresponsive and called 911. She presented to the Emergency Department as a STEMI Alert, and was in cardiogenic shock, with very poor perfusion. The ECG from the ED shows a large antero-lateral M.I., with ST elevation in V2 through V6, and also I and aVL. In addition, there are pathological Q waves, indicating necrosis, in the precordial leads, V2 through V6. The inferior wall leads, II, III, and aVF, also have pathological Q waves and abnormally shaped ST segments - no longer distinctly elevated, but coved upward.
This is a good tracing to teach students about Q waves and "old", "new", and "recent" M.I., and also about the clinical effects of hypokinesis or akinesis of the ventricles.
Unfortunately, this patient suffered a cardiac arrest in the cath lab while having her LCA reperfused with balloon angioplasty. She was resuscitated, on a ventilator and intraaortic balloon pump, and admitted to the CVICU, where she passed away within a few hours.
You will find photos from her cardiac cath in the Other Instructor Resources section, labelled as patient AW103. Click here for RCA Image, LCA Occluded Image, LCA Angioplasty Image. Videos of her ventriculogram and left coronary artery angiogram can be found in the Resources section of this website.