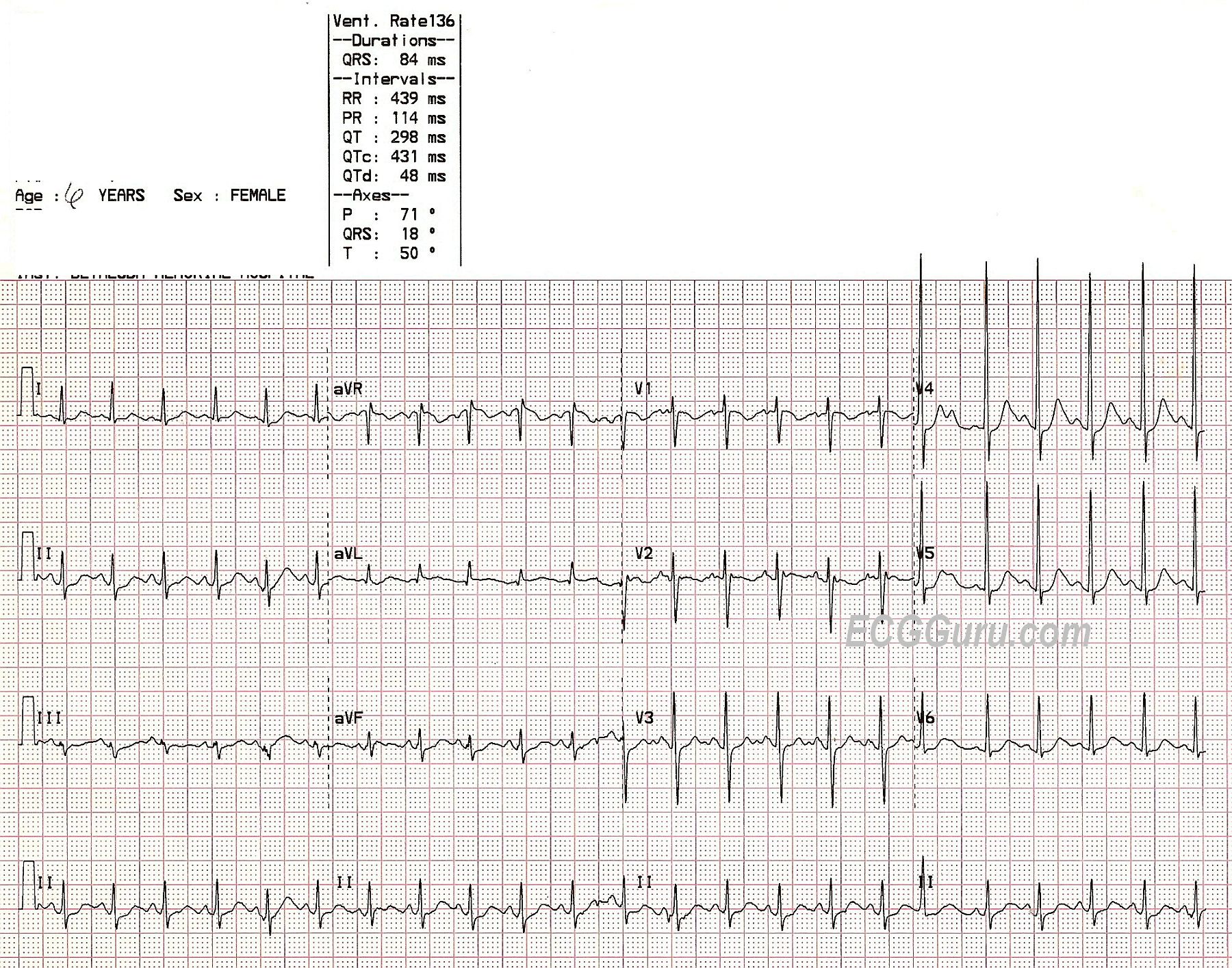
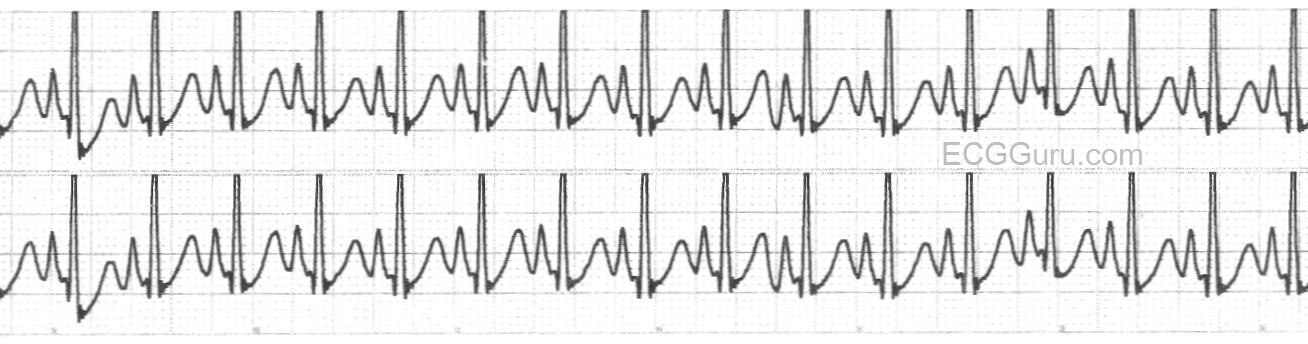
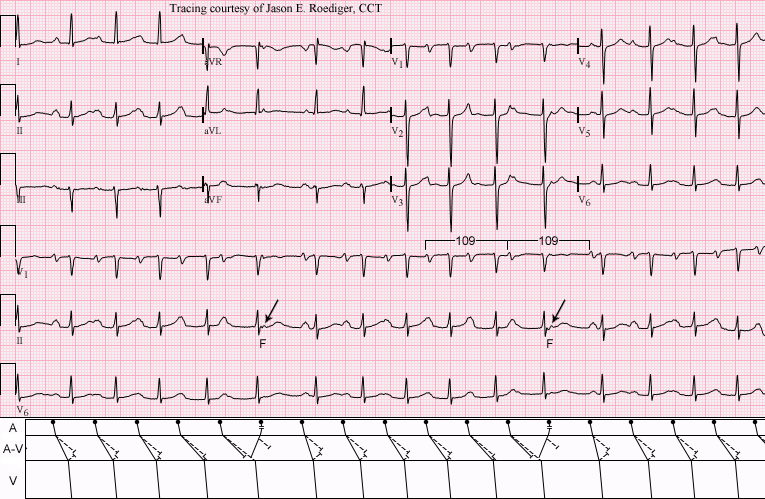
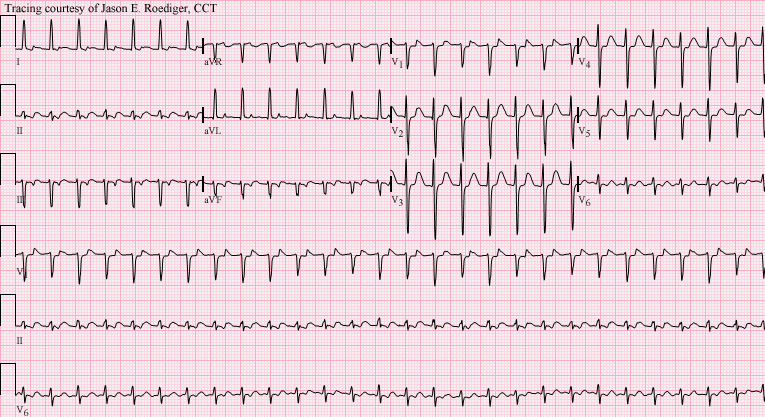
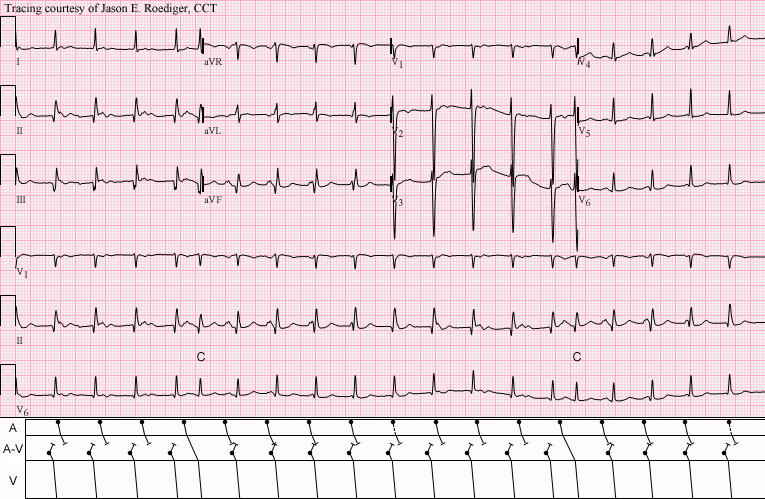
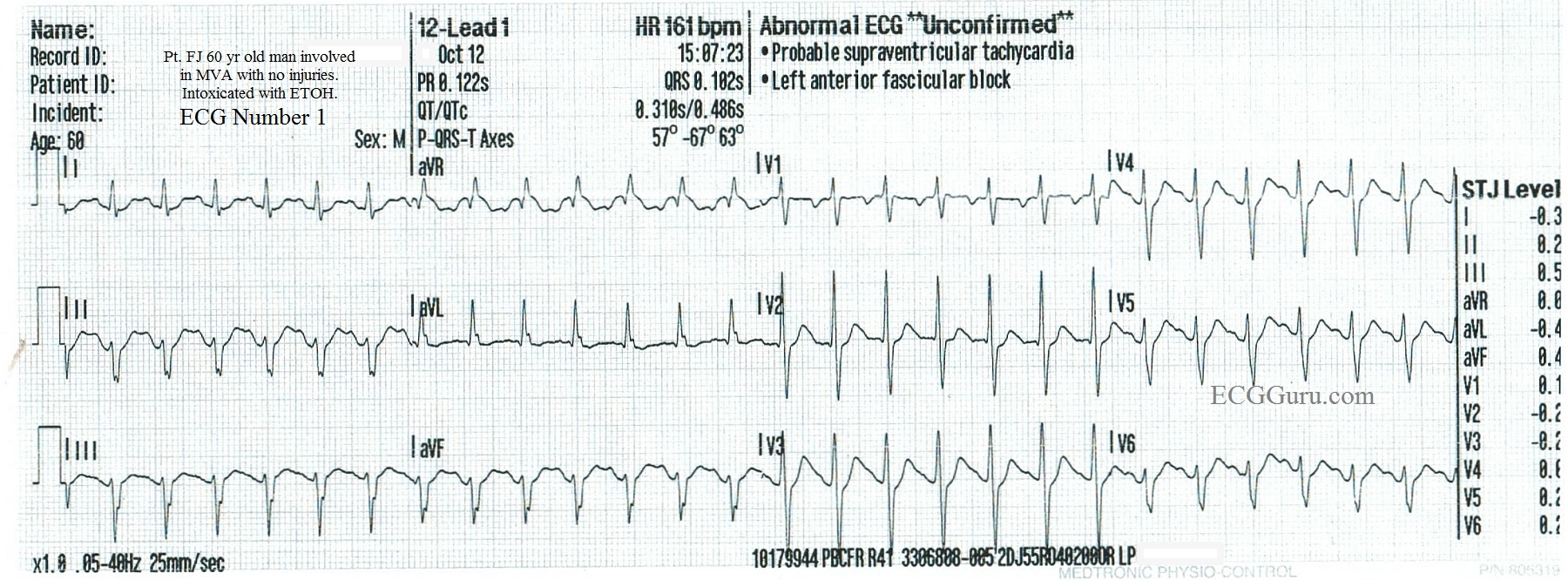
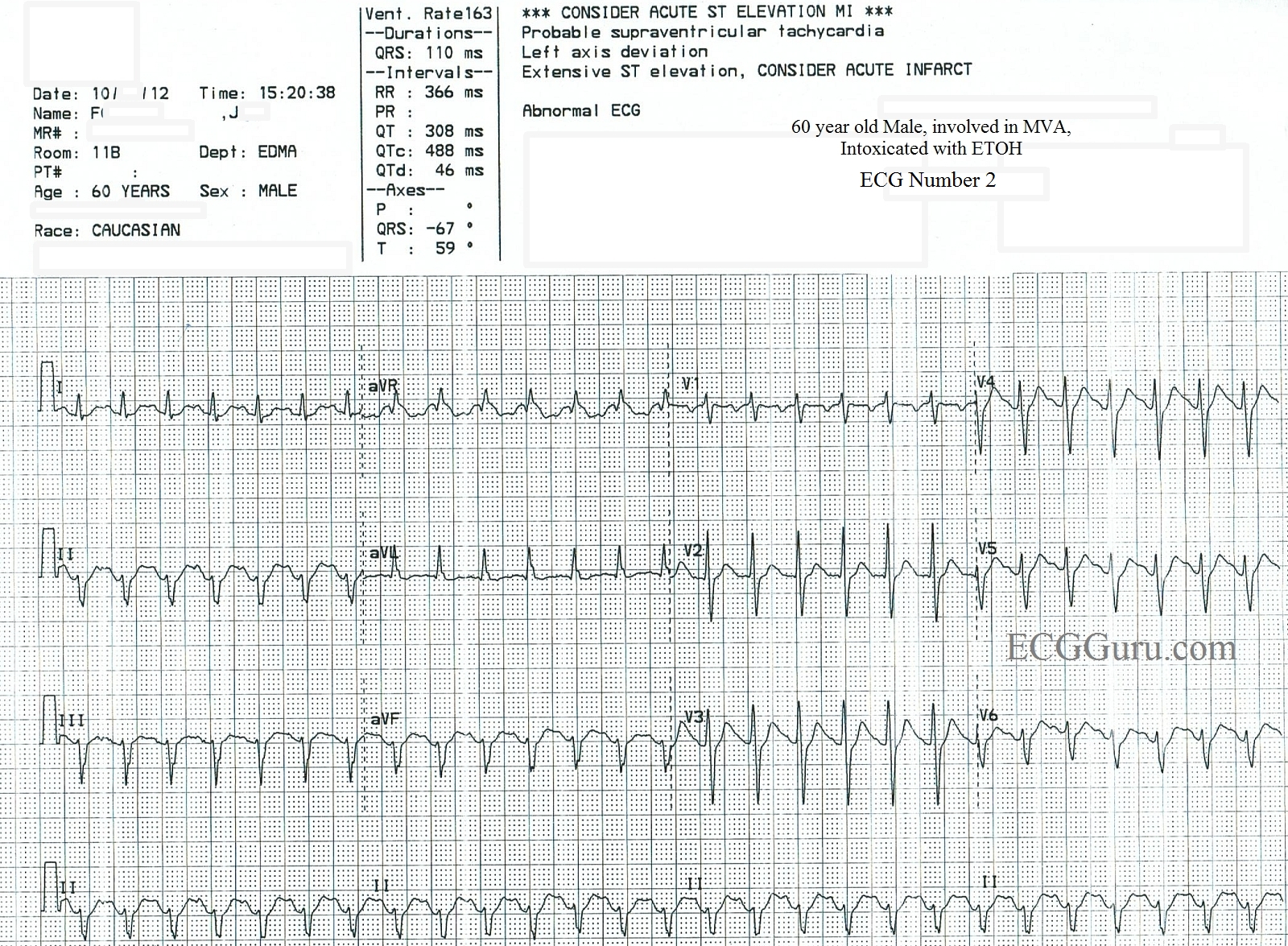
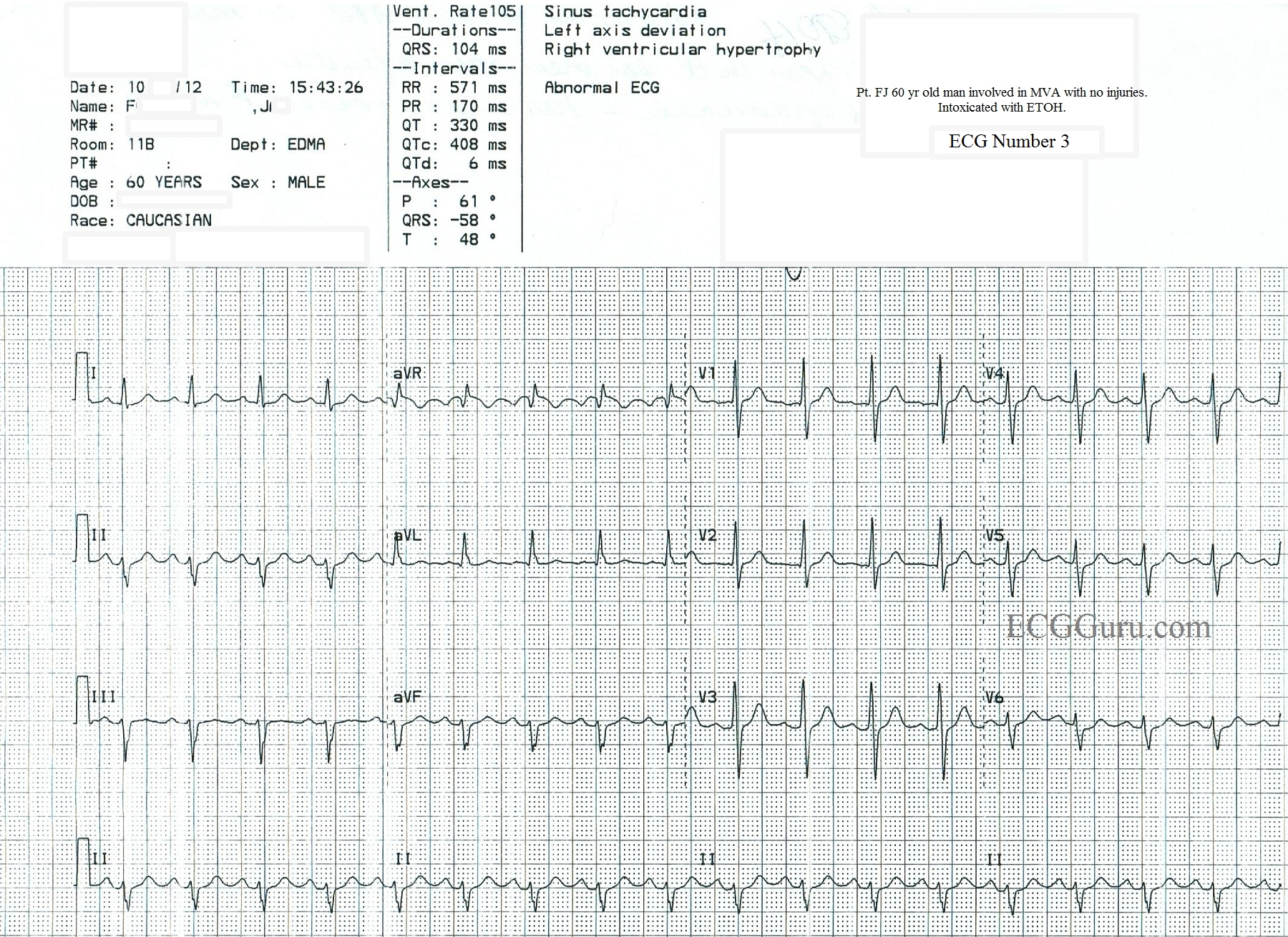
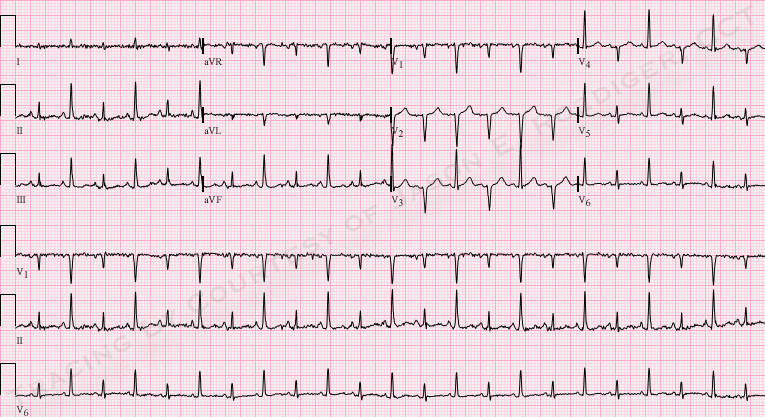
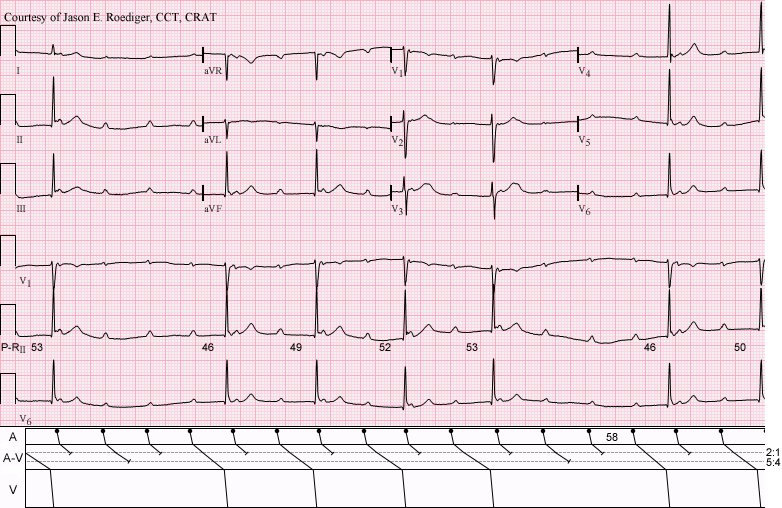
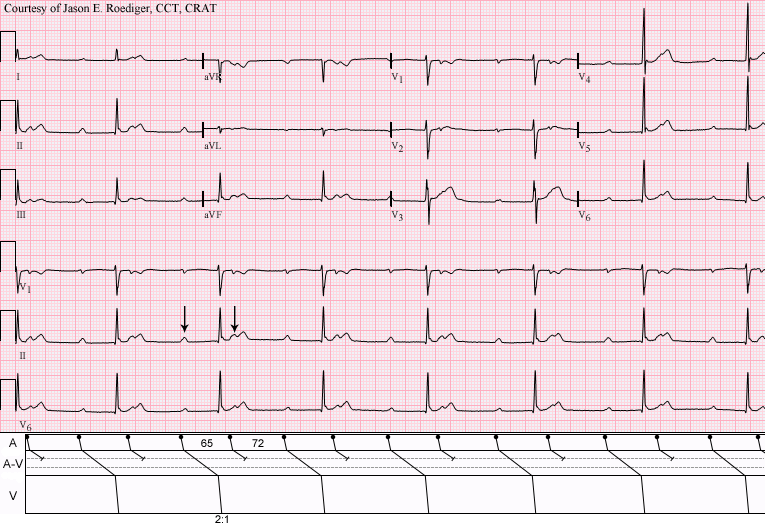
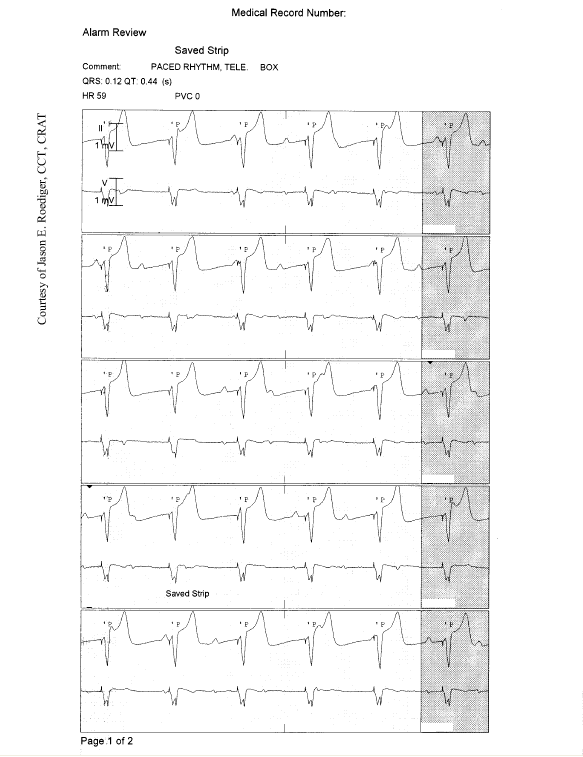
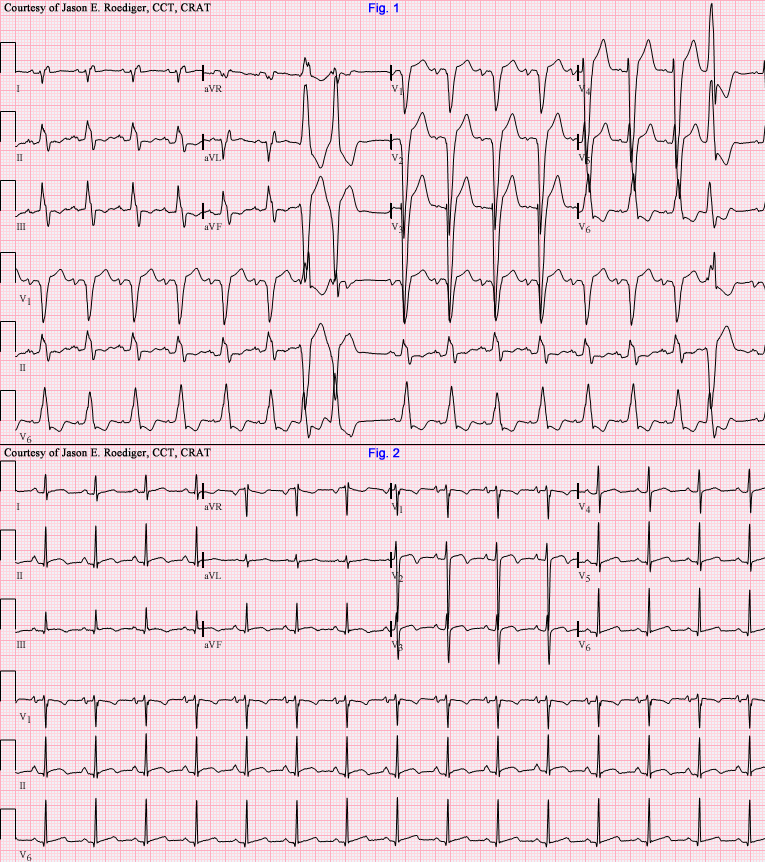
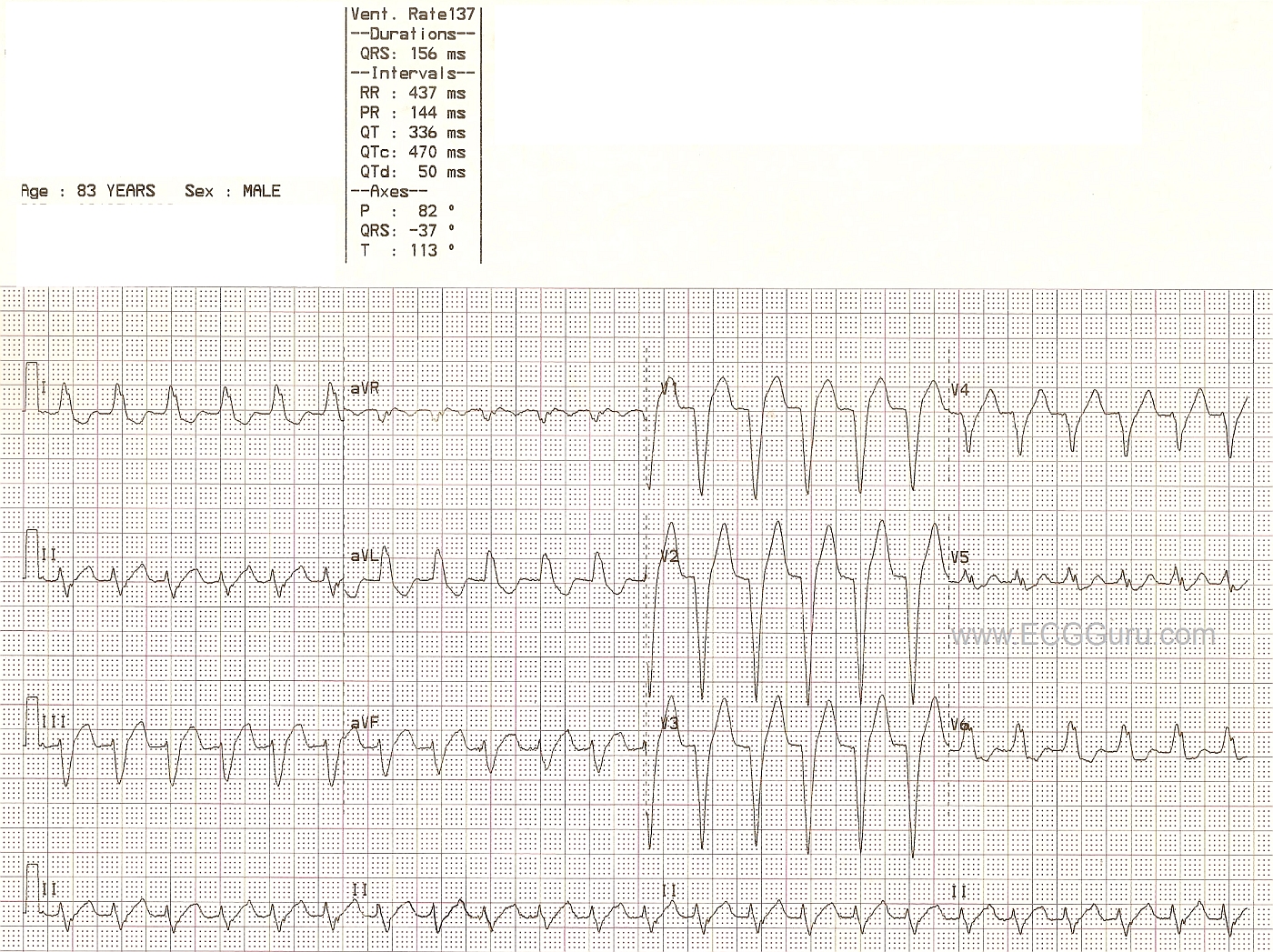
This series of ECGs was obtained from a 60-year-old man who was involved in a one-car accident. He sustained no injuries, but his blood alcohol level was far above the legal limit for intoxication at over 300 mmol/L. ECG No. 1 shows the ECG obtained by paramedics in the field, which they incorrectly interpreted to be atrial fibrillation. No medication was given. The ER physician obtained ECG No. 2, and considered sinus tachycardia as the diagnosis, but also, because of the fast rate and the fact that the rate had not changed for at least 15 minutes, he considered SVT or atrial flutter with 2:1 conduction. The ERP administered diltiazem (Cardizem) to the patient, which resulted in ECG No. 3. The transition to the slower rate was not captured on rhythm strips, but the nurse's notes showed a gradual change over 15 minutes from a rate of 160 to 105/min.
Usually, on the Instructors' Collection ECGs, we like to give the "answer". In this case, however, there will undoubtedly be some discussion regarding what went on. This discussion can be useful if you are teaching intermediate to advanced students. Questions to consider: 1) Is the fast rhythm an SVT and, if so, which one? 2) Is it sinus tachycardia and, if so, what are the effects of the car accident and the alcohol? 3) Is the left anterior fascicular block relevant? (Criteria are left axis deviation, slightly widened QRS complex at 110 ms, no other obvious reason for the axis deviation). 4) Is the ST elevation in the inferior wall during the tachycardia a sign of acute M.I.? The patient was lost to followup, so it is not known whether the ST changes were investigated. Note the flat ST segment and inverted T waves in V1 during the tachycardia that resolve when the rate decreases.
Please log in to register your comments on this interesting series.