Submitted by Dr A Röschl on Thu, 04/24/2025 - 01:13
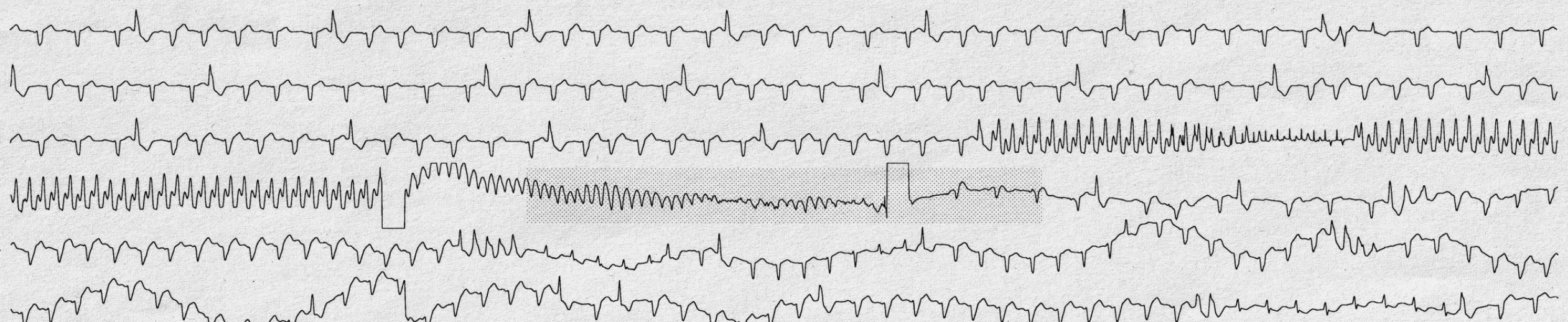
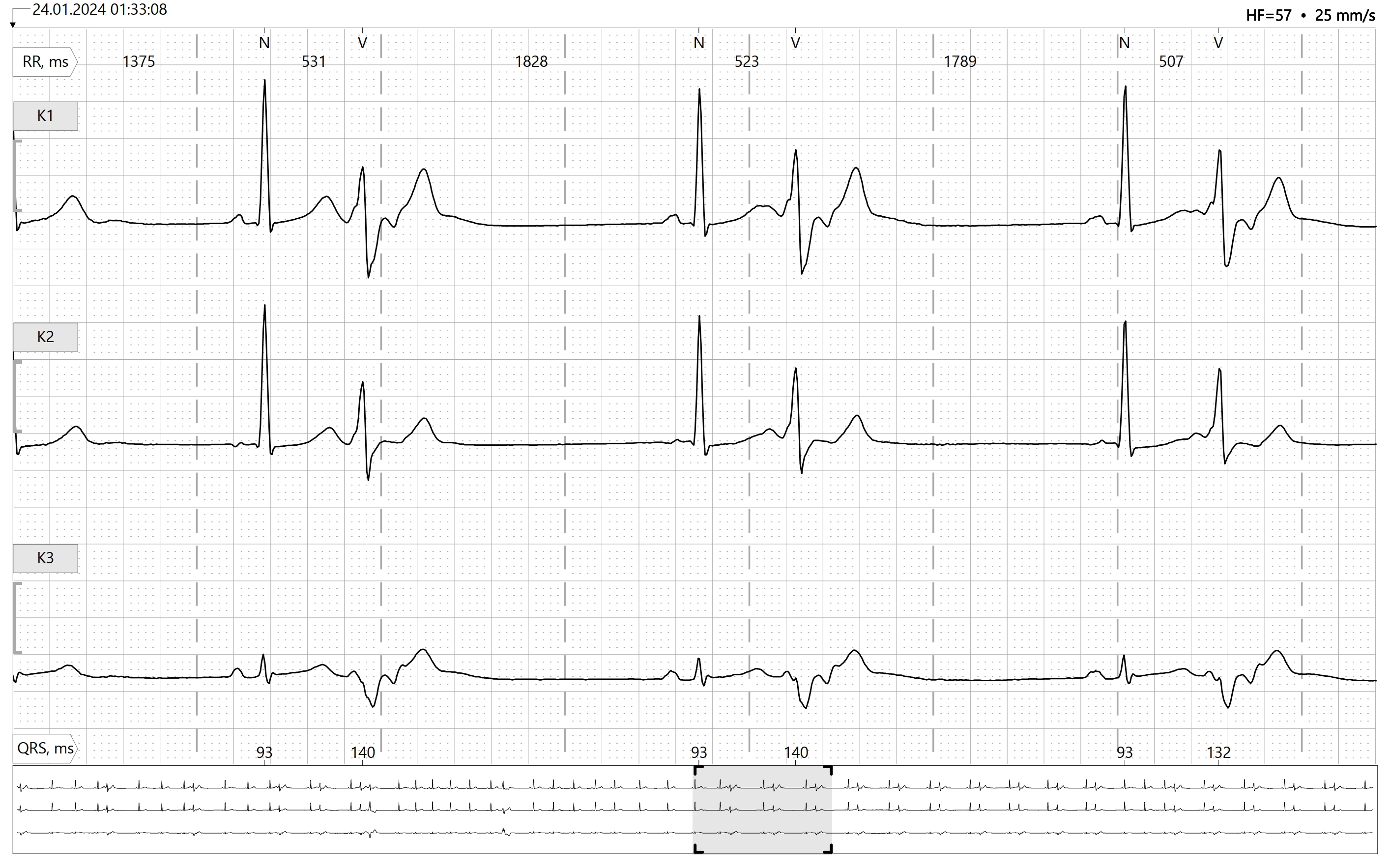
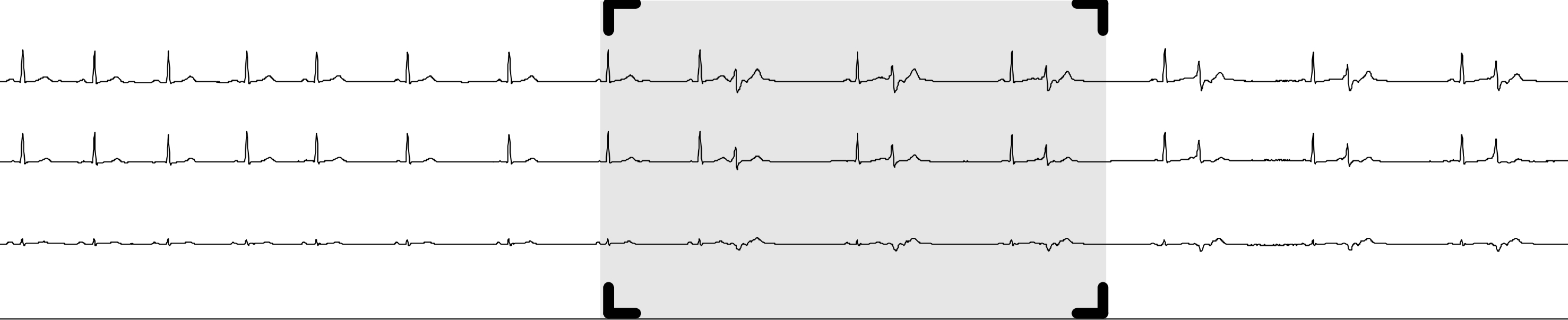
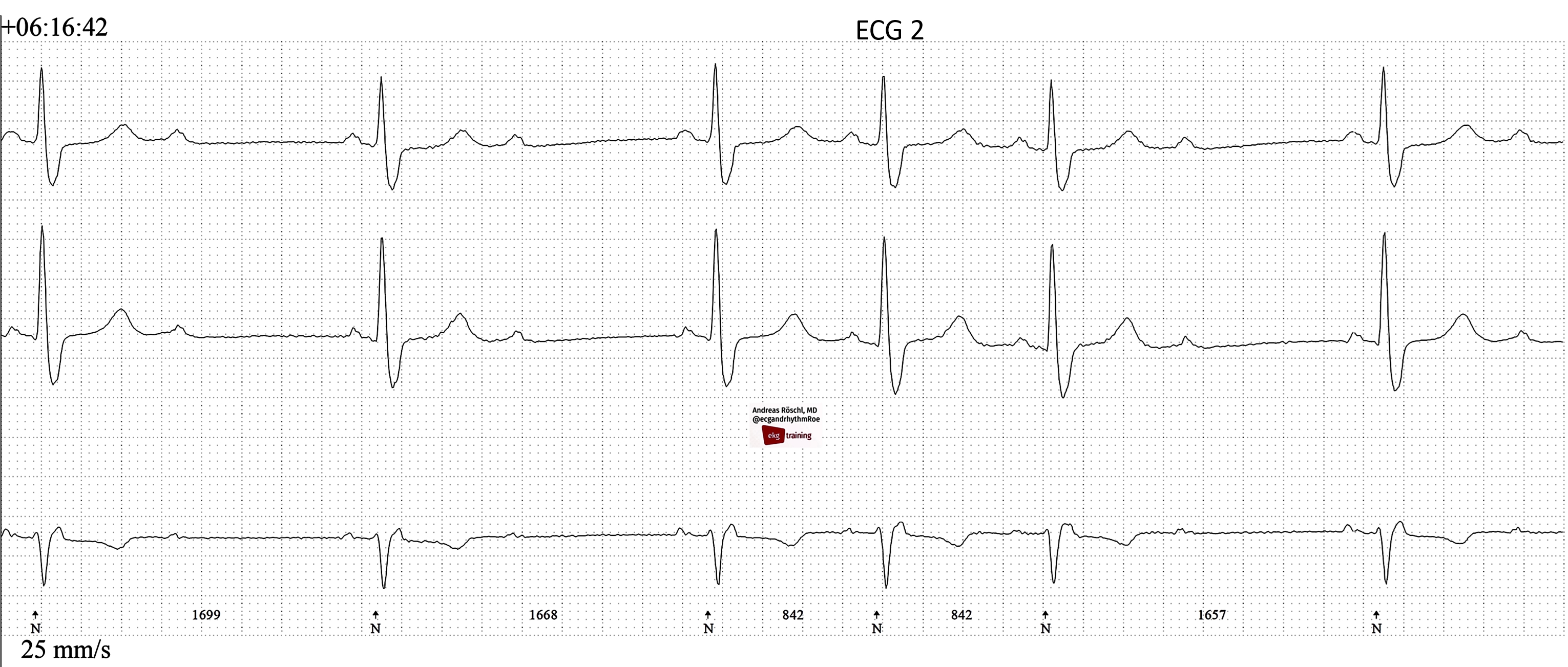
Sometimes a single Holter ECG can tell a whole story. Here we see a single-channel ECG, each line representing about 30 seconds.
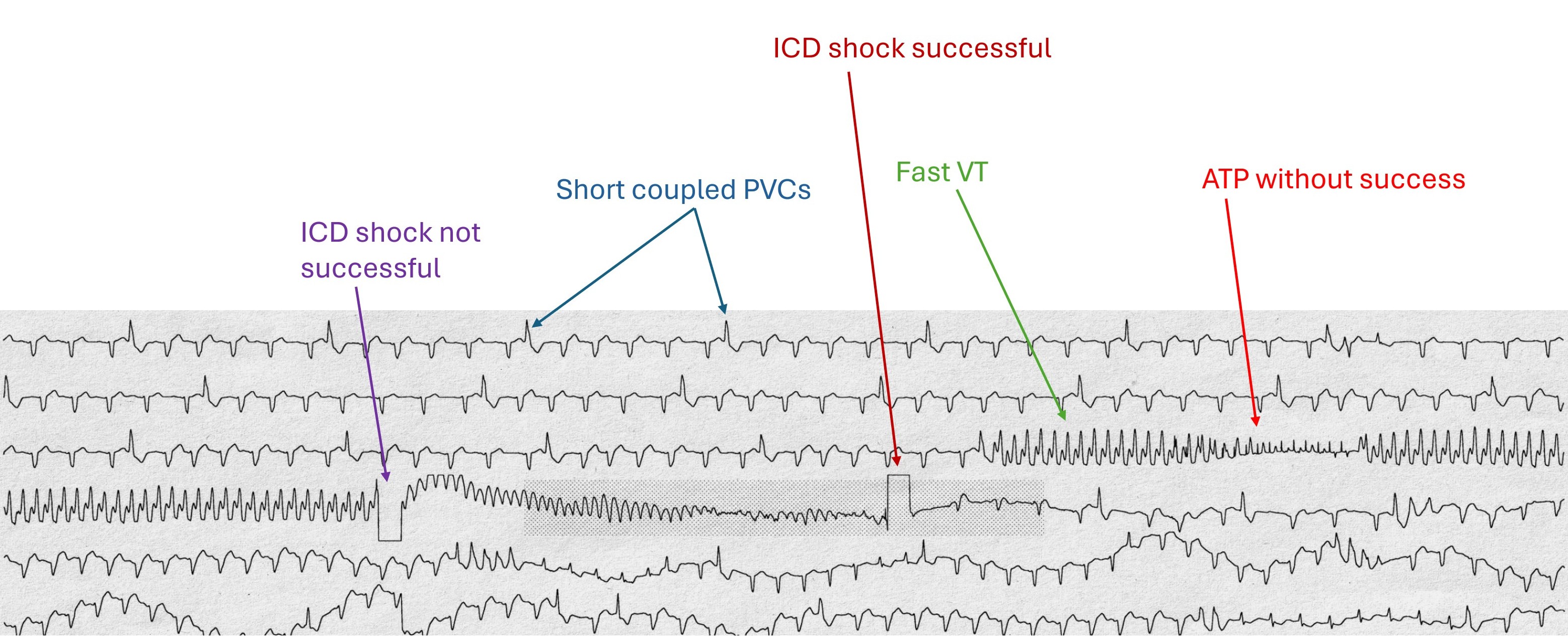
The ECG is from a 56-year-old man with severe ischemic cardiomyopathy who had an ICD implanted a few months ago due to recurrent ventricular tachycardia.
The explanation of what can be seen on this ECG can be found on the 2nd image.
Interestingly, the patient did not notice these events, they had occurred at night during sleep.
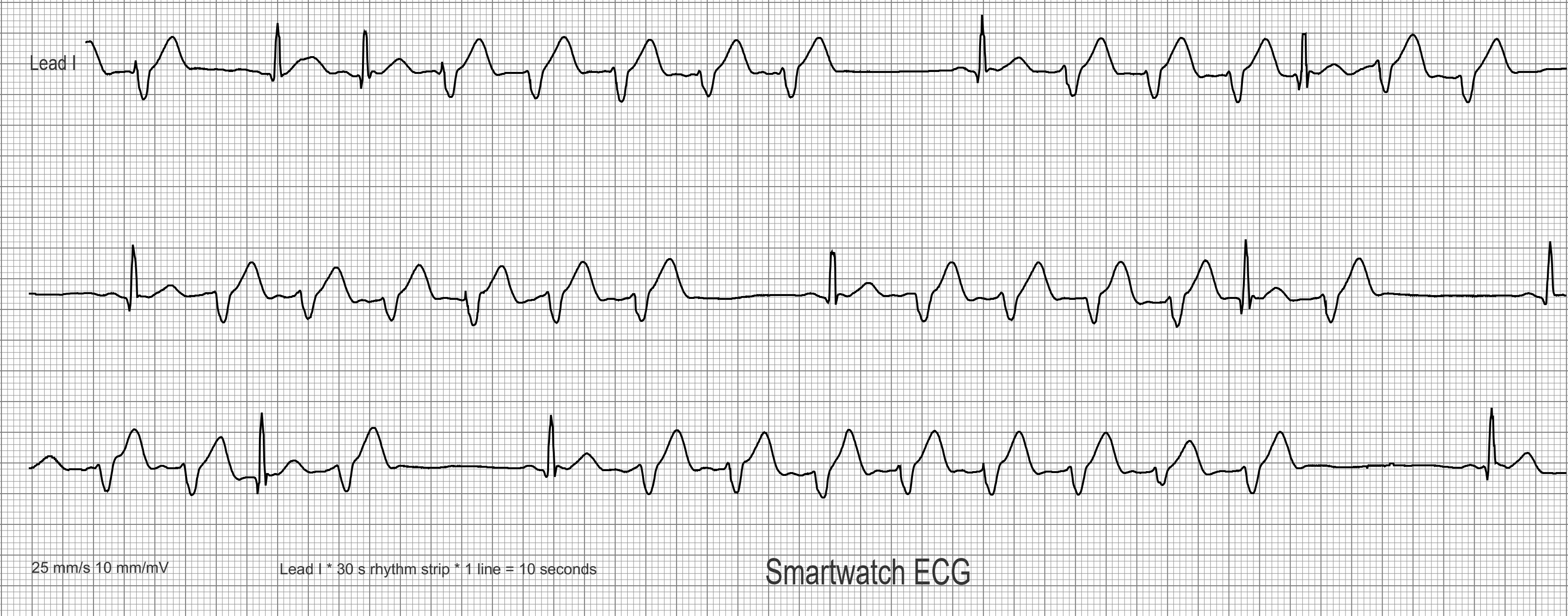
Submitted by Dr A Röschl on Fri, 01/03/2025 - 02:39
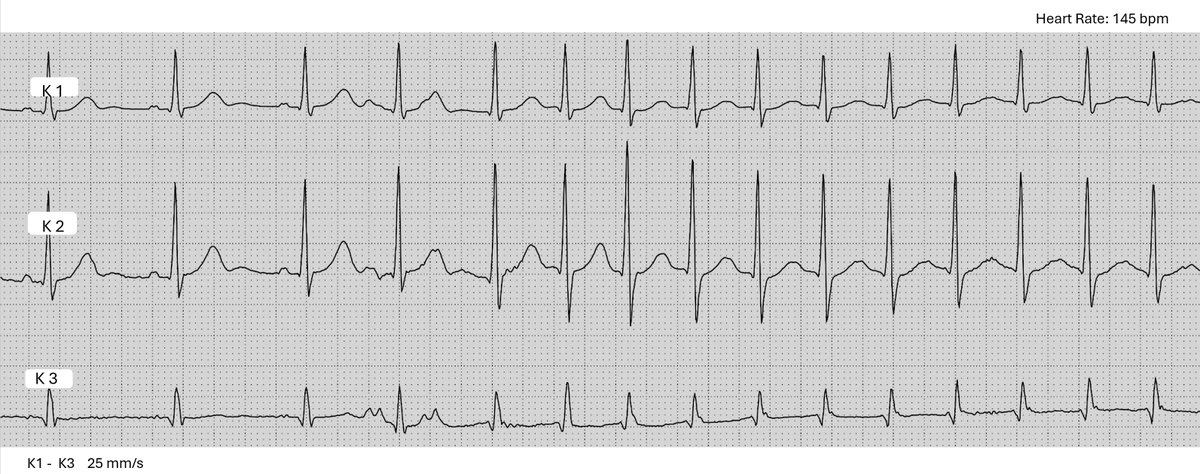
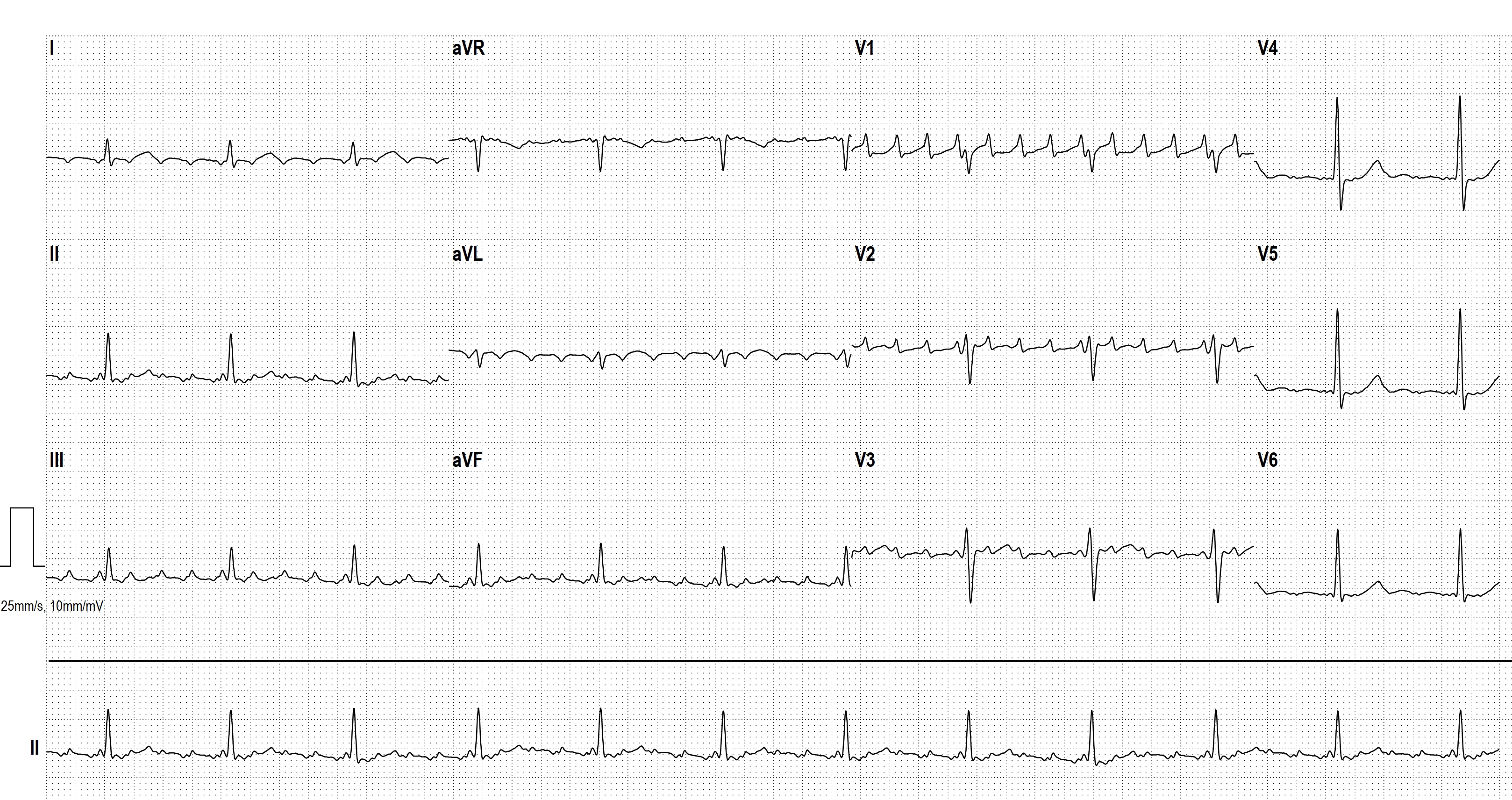
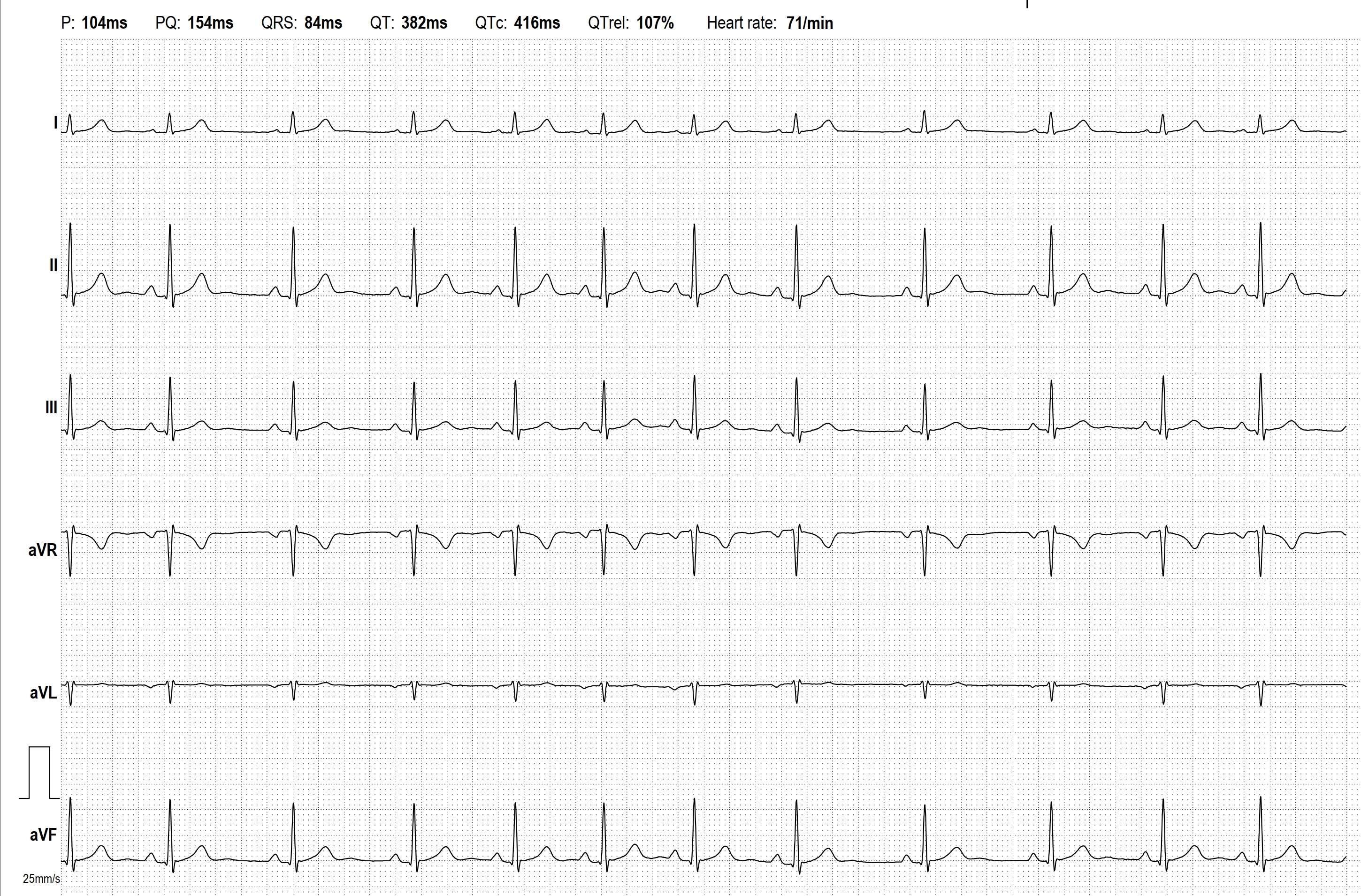
Here we see a 30 s long strip of a 1-lead ECG rhythm strip, recorded with a modern Smartwatch (Apple watch). The ECG has been graphically processed for better visualization. The paper speed is 25 mm/s as usual. The lead shown corresponds to ECG lead I of the limb leads.
Submitted by Dr A Röschl on Sun, 08/25/2024 - 02:04
Sometimes you see an ECG strip, look at it and then put it away again with the thought: I don't understand this. But if you take your time and analyze the ECG systematically, you will usually come to a good result. This is an example of such an ECG (certainly not the most difficult). The explanation is shown in the 2nd picture.
Submitted by Dr A Röschl on Tue, 07/30/2024 - 03:13
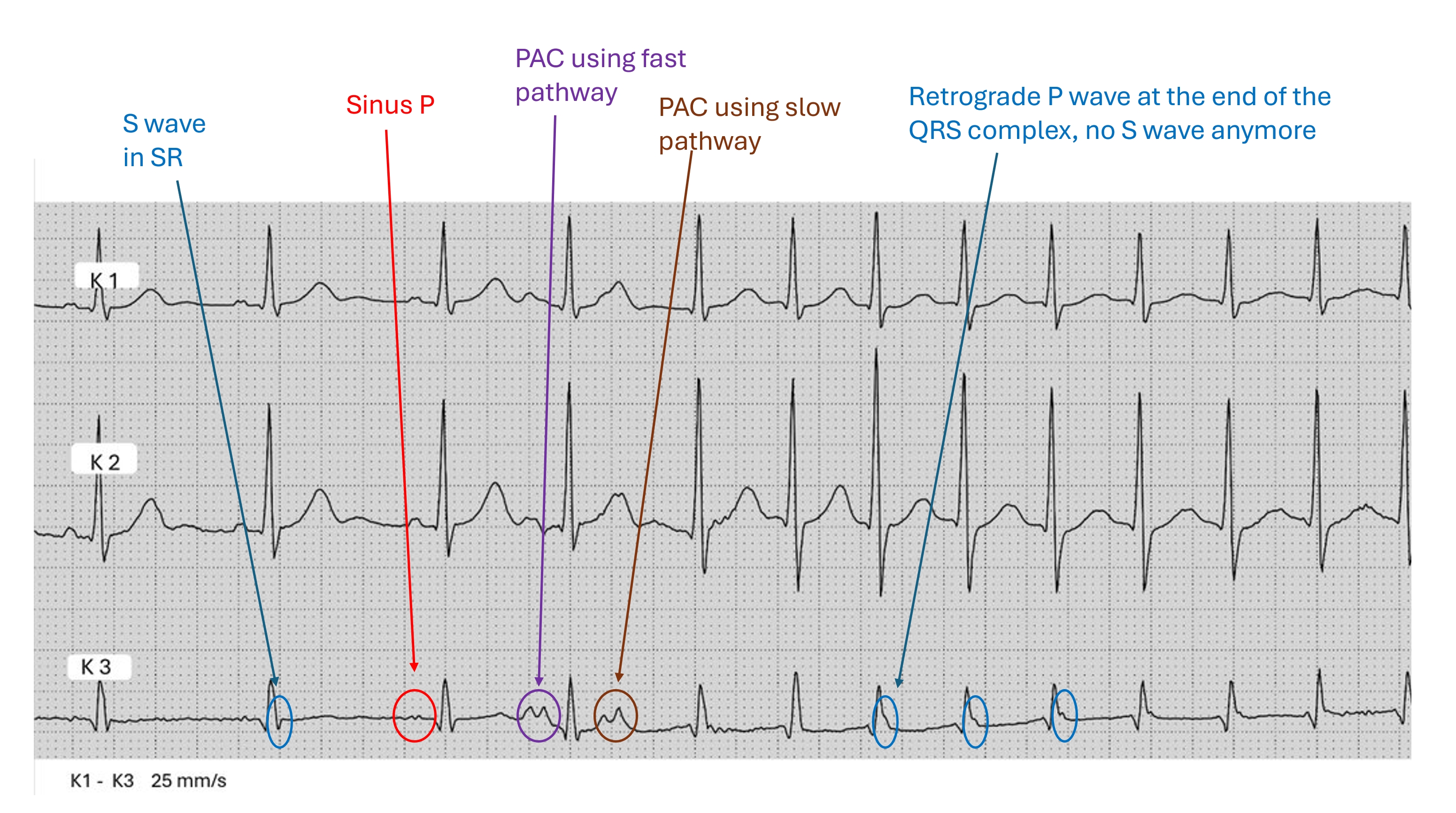
The first 3 beats are sinus node beats, all have the same morphology of the P wave. This is followed by a PAC, which is conducted via the fast pathway in the AV node. The next PAC is conducted via the slow pathway, then the AV nodal reentry tachycardia (slow/fast) starts. The retrograde P waves are visible at the end of the QRS complex in the lower lead K3.
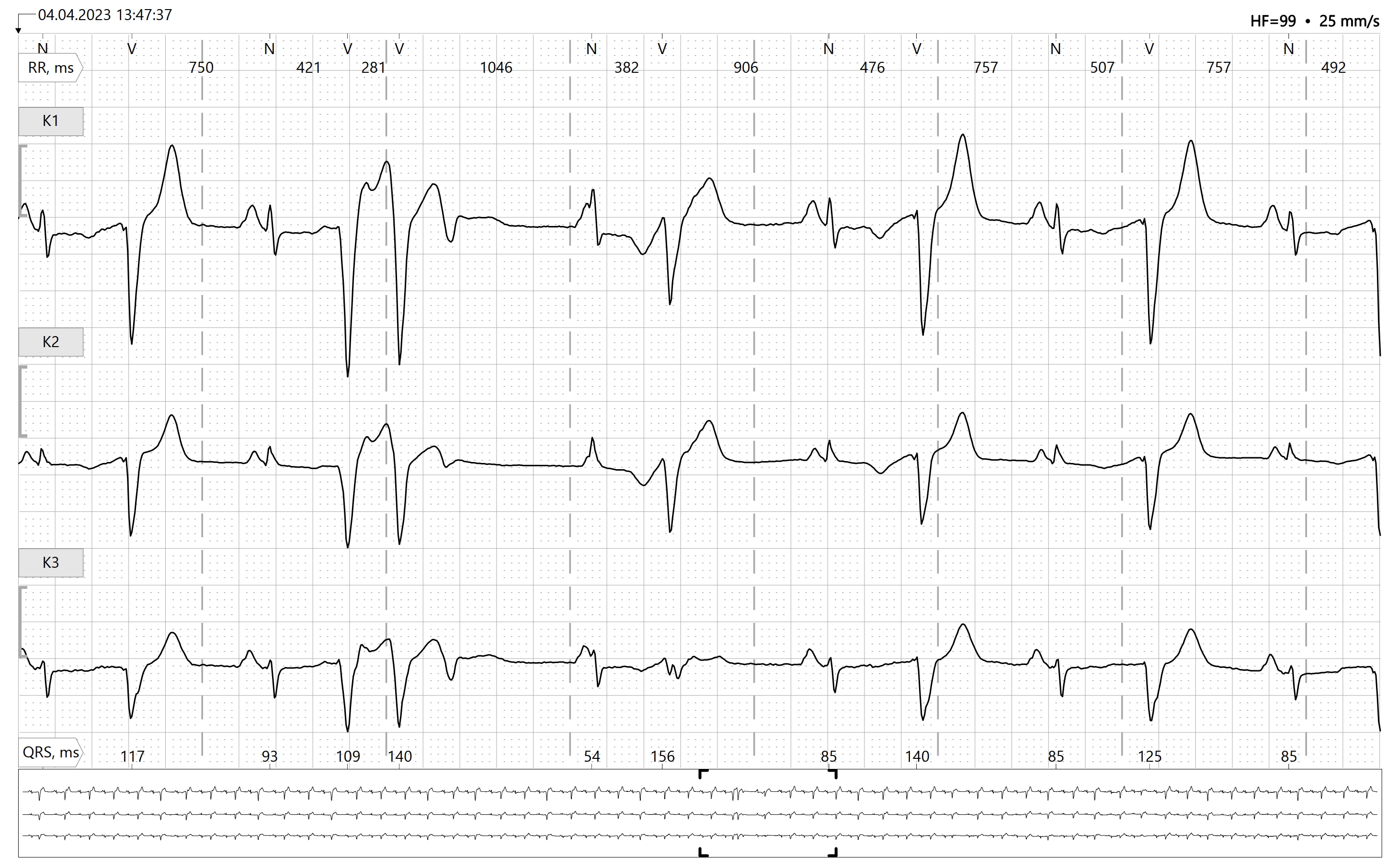
Submitted by Dr A Röschl on Sat, 07/27/2024 - 04:06
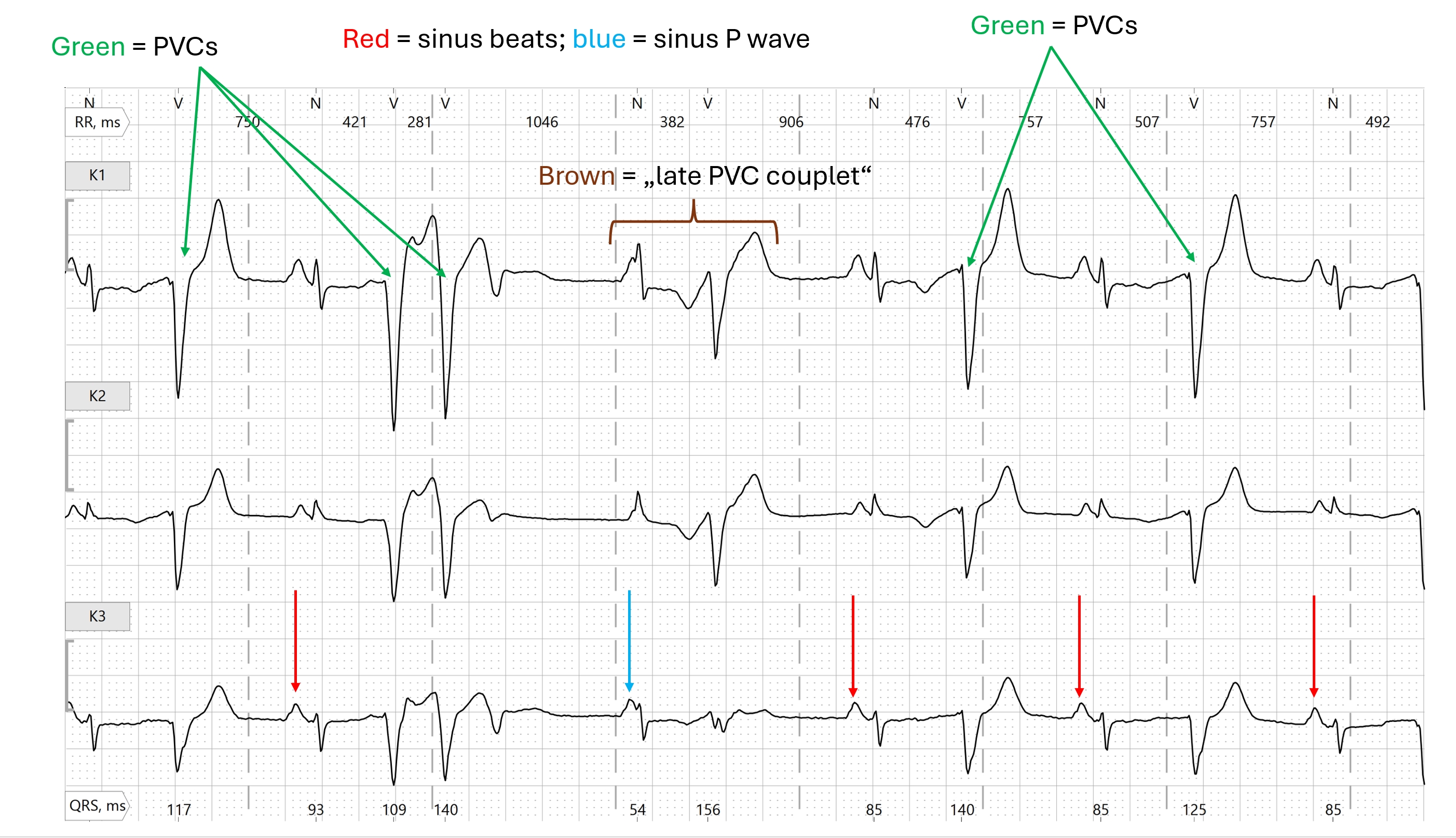
Why is the pause after the PVCs relatively long? We see a sinus arrhythmia in the rhythm strip. The ventricular extrasystoles penetrate the AV node retrogradely and reset the sinus rhythm, which then restarts. VA conduction can be recognized by the inverted P wave following the QRS complex of the ventricular extrasystole (PVC).
Submitted by Dr A Röschl on Mon, 12/11/2023 - 01:07
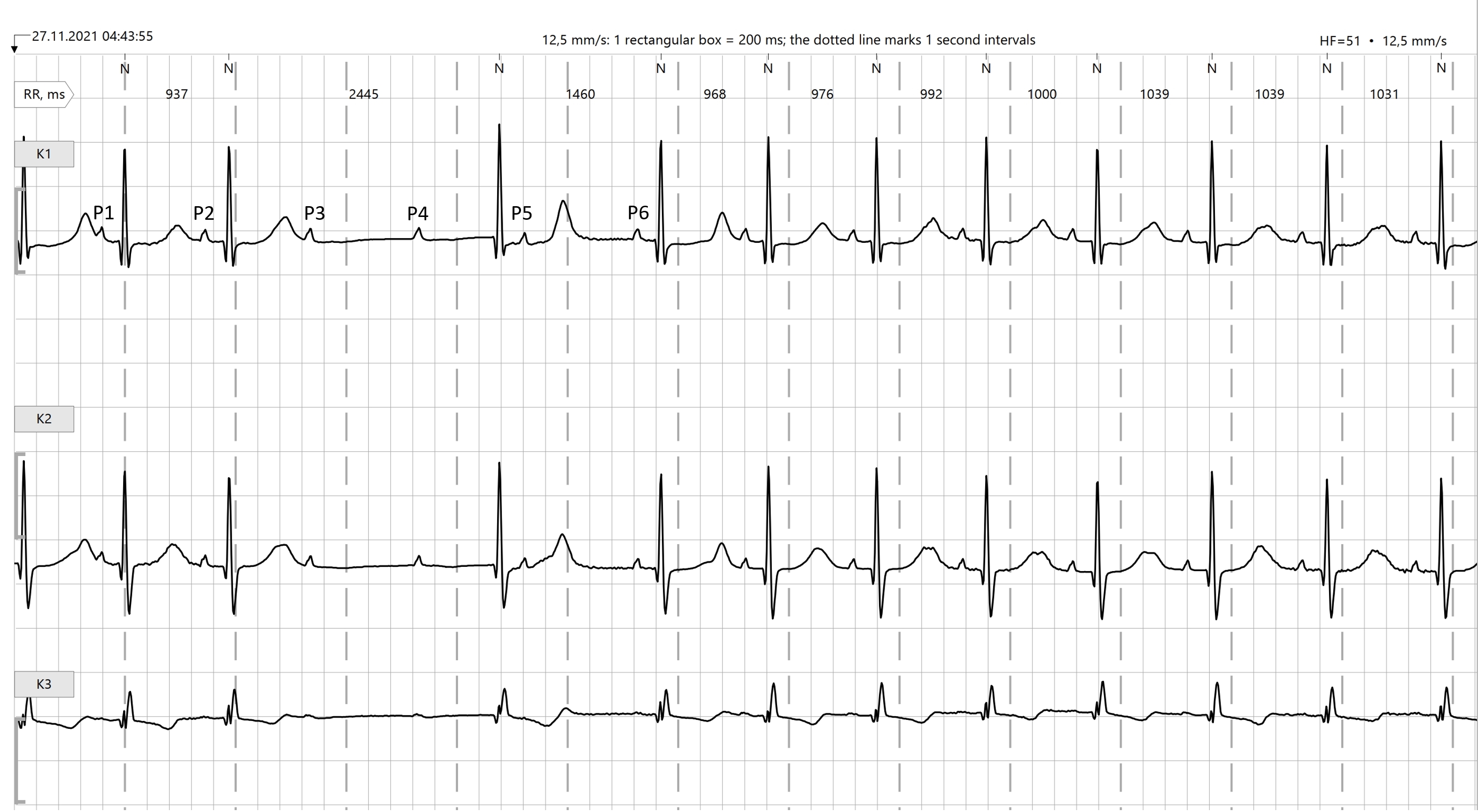
Why is this a high-grade AV block? If at least 3 P-waves are not conduced and there is normal AV conduction before and after, this can be considered a high-grade AV block. In this Holter strip, P1, P2 and all P-waves from P6 onwards are conducted, albeit with a prolonged PR interval (first-degree AV block). P3, P4, P5 are not conducted. A junctional escape beat is seen before P5. P5 can also not be conducted because the specific conduction system is still refractory at this time due to the junctional escape beat.
Submitted by Dr A Röschl on Mon, 12/11/2023 - 00:43
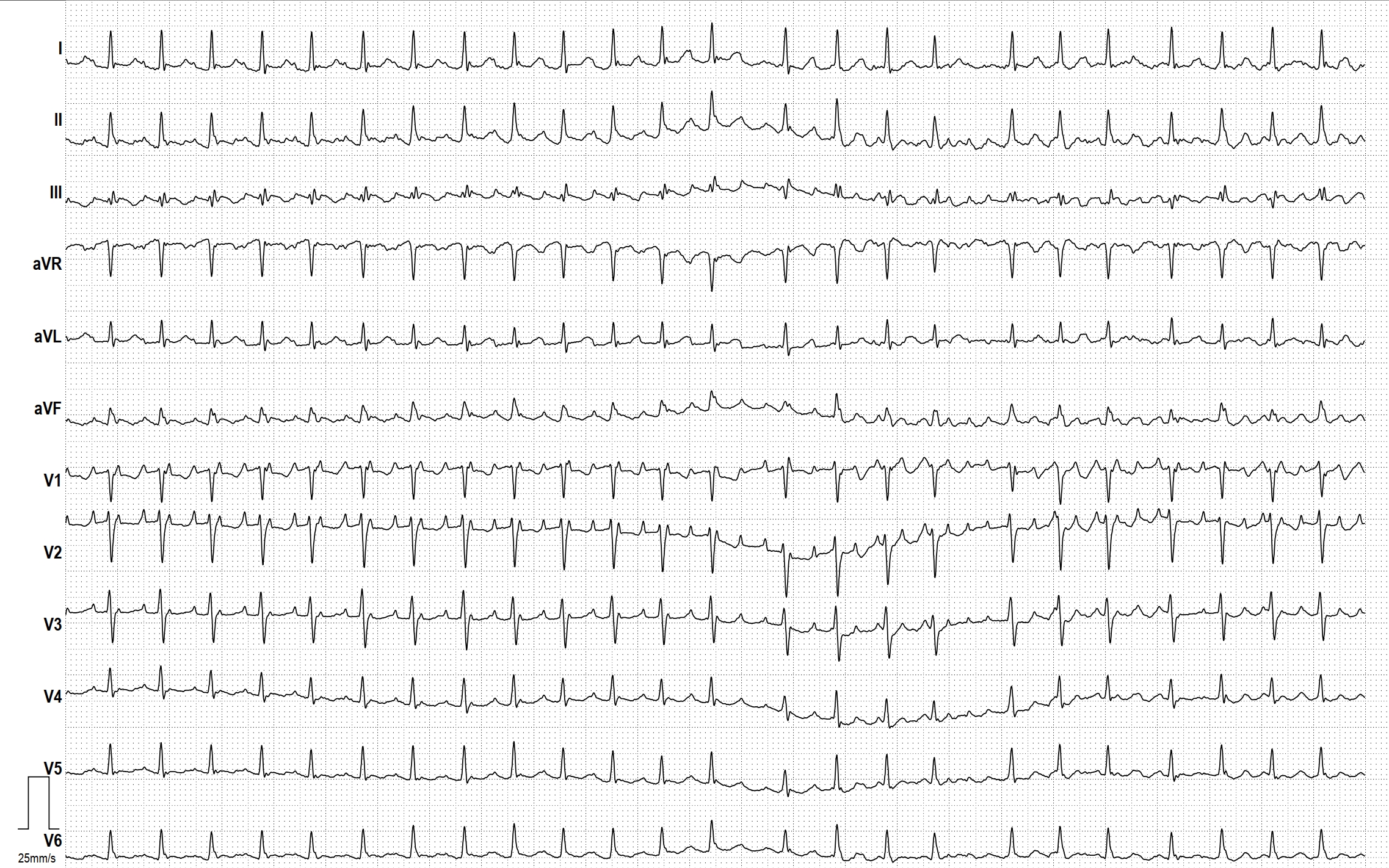
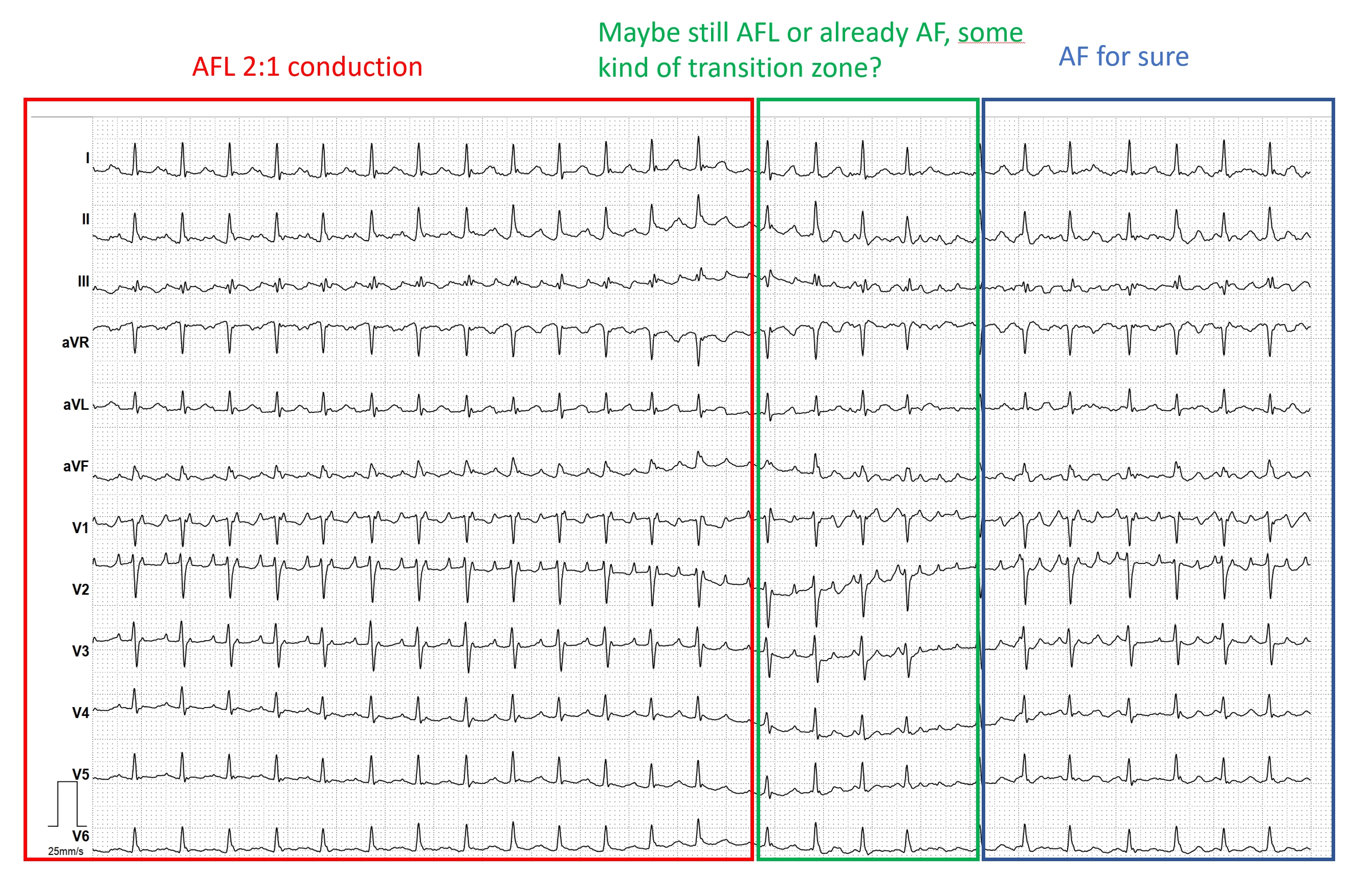
Atrial flutter and atrial fibrillation are two different cardiac arrhythmias, but occur frequently side by side in the same patient. Here is an example of how atrial flutter degenerataes into atrial fibrillation. The initially ordered atrial activity (left in the picture) with 2 flutter waves/1 QRS complex changes into irregular atrial activity (right in the picture) and the RR intervals become completely irregular.
Submitted by Dr A Röschl on Thu, 08/10/2023 - 01:07
Here we see the EKG of a 15-year-old girl. The rhythm is irregular, with the heart rate fluctuating between approximately 60 and 90 beats per minute. All P waves are identical, and the PR interval is always constant. Therefore, a sinus arrhythmia is present. In this case, it is a respiratory sinus arrhythmia, which is commonly found in younger individuals. The heart rate increases reflexively during inspiration and decreases during exspiration. This physiological sinus arrhythmia is usually no longer present in older individuals.
Submitted by Dr A Röschl on Wed, 08/02/2023 - 02:35
We are observing EKG strip 1 in a Holter EKG recording; what can be said about it? There is a sinus rhythm with a normal PQ interval. After 3 sinus beats, a 2:1 AV block develops. When 2:1 AV block occurs, we should not refer to this as Wenckebach (Mobitz I) or Mobitz II, but rather as a high-grade AV block (other forms include: 3:1, 4:1, 5:1, etc.). The 2:1 block can be intranodally localized and behave benignly like a Wenckebach block typically does. However, it could also be infranodally localized with a potentially serious prognosis.